

Lung Ultrasound for Identification of Patients Requiring Invasive Mechanical Ventilation in COVID-19
- PMID: 33496362
- PMCID: PMC8014139
- DOI: 10.1002/jum.15617
Lung Ultrasound for Identification of Patients Requiring Invasive Mechanical Ventilation in COVID-19
Abstract
Objectives: Indication for invasive mechanical ventilation in COVID-19 pneumonia has been a major challenge. This study aimed to evaluate if lung ultrasound (LUS) can assist identification of requirement of invasive mechanical ventilation in moderate to severe COVID-19 pneumonia.
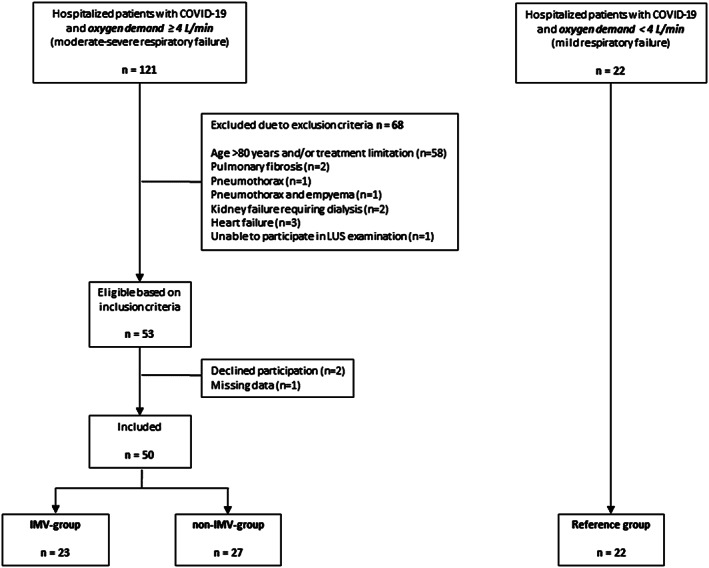
Materials and methods: Between April 23 and November 12, 2020, hospitalized patients with moderate to severe COVID-19 (oxygen demand ≥4 L/min) were included consecutively. Lung ultrasound was performed daily until invasive mechanical ventilation (IMV-group) or spontaneous recovery (non-IMV-group). Clinical parameters and lung ultrasound findings were compared between groups, at intubation (IMV-group) and highest oxygen demand (non-IMV-group). A reference group with oxygen demand <4 L/min was examined at hospital admission.
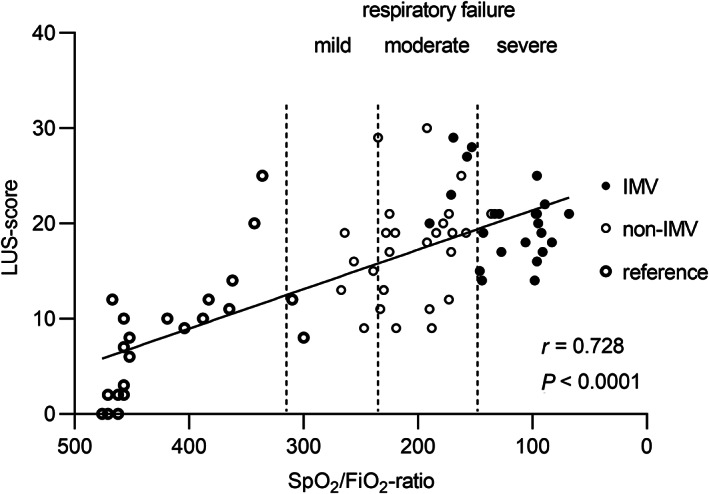
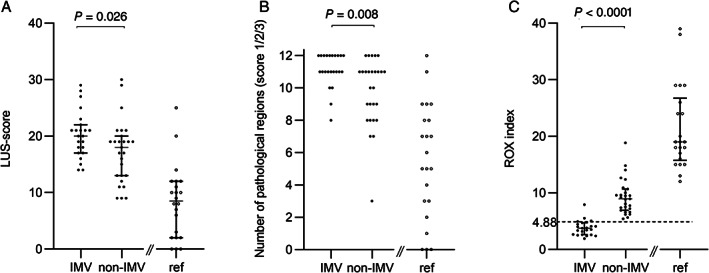
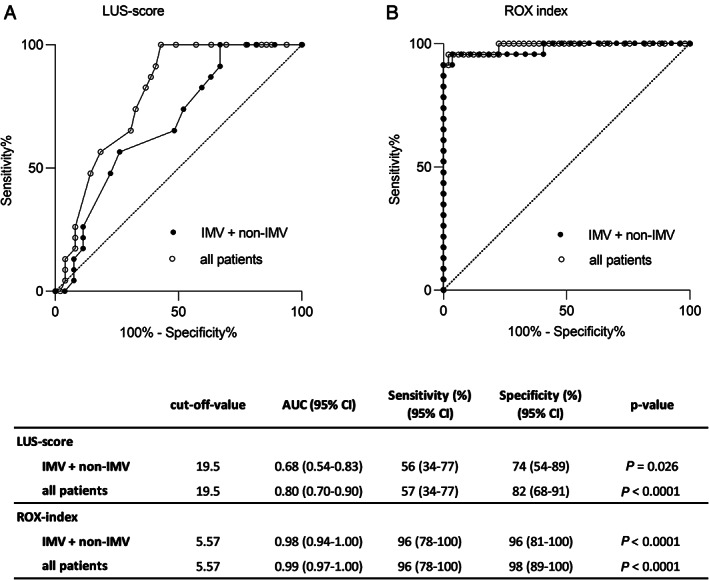
Results: Altogether 72 patients were included: 50 study patients (IMV-group, n = 23; non-IMV-group, n = 27) and 22 reference patients. LUS-score correlated to oxygen demand (SpO2 /FiO2 -ratio) (r = 0.728; p < .0001) and was higher in the IMV-group compared to the non-IMV-group (20.0 versus 18.0; p = .026). Based on receiver operating characteristic analysis, a LUS-score of 19.5 was identified as cut-off for requirement of invasive mechanical ventilation (area under the curve 0.68; sensitivity 56%, specificity 74%). In 6 patients, LUS identified critical coexisting conditions. Respiratory rate and oxygenation index ((SpO2 /FiO2 )/respiratory rate) ≥4.88 identified no requirement of invasive mechanical ventilation with a positive predictive value of 87% and negative predictive value of 100%.
Conclusions: LUS-score had only a moderate diagnostic value for requirement of invasive mechanical ventilation in moderate to severe COVID-19. However, LUS proved valuable as complement to respiratory parameters in guidance of disease severity and identifying critical coexisting conditions.
Keywords: COVID-19; Coronavirus; mechanical; ultrasonography; ventilators.
© 2021 The Authors. Journal of Ultrasound in Medicine published by Wiley Periodicals LLC. on behalf of American Institute of Ultrasound in Medicine.
Figures
References
-
- World Health Organization timeline : WHO's COVID‐19 response. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019/interact...
-
- Brochard L, Slutsky A, Pesenti A. Mechanical ventilation to minimize progression of lung injury in acute respiratory failure. Am J Respir Crit Care Med 2017; 195:438–442. - PubMed
-
- Volpicelli G, Elbarbary M, Blaivas M, et al. International evidence‐based recommendations for point‐of‐care lung ultrasound. Intensive Care Med 2012; 38:577–591. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
