

A randomized porcine study of the hemodynamic and metabolic effects of combined endovascular occlusion of the vena cava and the aorta in normovolemia and in hemorrhagic shock
- PMID: 33496552
- PMCID: PMC8081444
- DOI: 10.1097/TA.0000000000003098
A randomized porcine study of the hemodynamic and metabolic effects of combined endovascular occlusion of the vena cava and the aorta in normovolemia and in hemorrhagic shock
Abstract
Background: Mortality from traumatic retrohepatic venous injuries is high and methods for temporary circulatory stabilization are needed. We investigated survival and hemodynamic and metabolic effects of resuscitative endovascular balloon occlusion of the aorta (REBOA) and vena cava inferior (REBOVC) in anesthetized pigs.
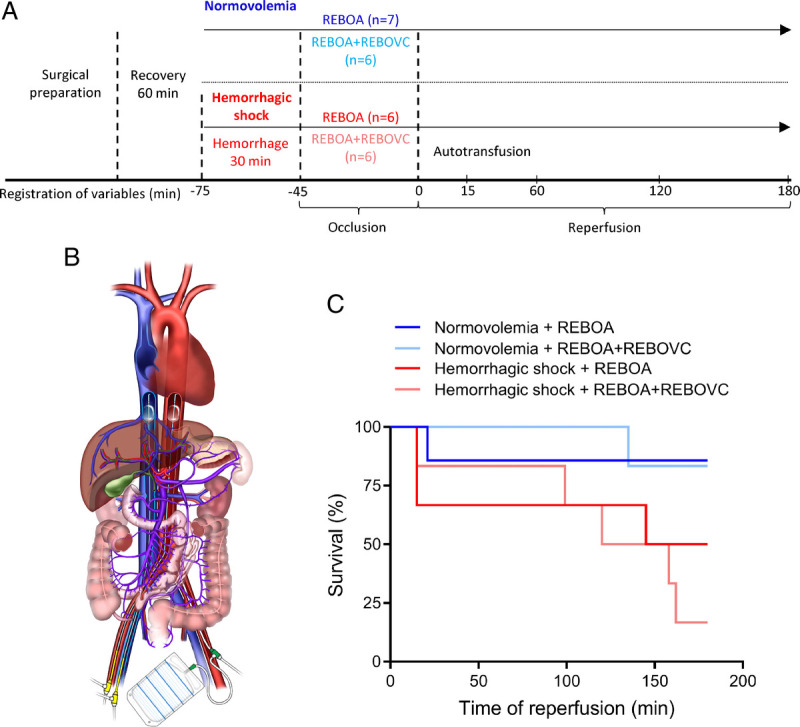
Methods: Twenty-five anesthetized pigs in normovolemia or severe hemorrhagic shock (controlled arterial bleeding in blood bags targeting systolic arterial pressure of 50 mm Hg, corresponding to 40-50% of the blood volume) were randomized to REBOA zone 1 or REBOA+REBOVC zone 1 (n = 6-7/group) for 45 minutes occlusion, followed by 3-hour resuscitation and reperfusion. Hemodynamic and metabolic variables and markers of end-organ damage were measured regularly.
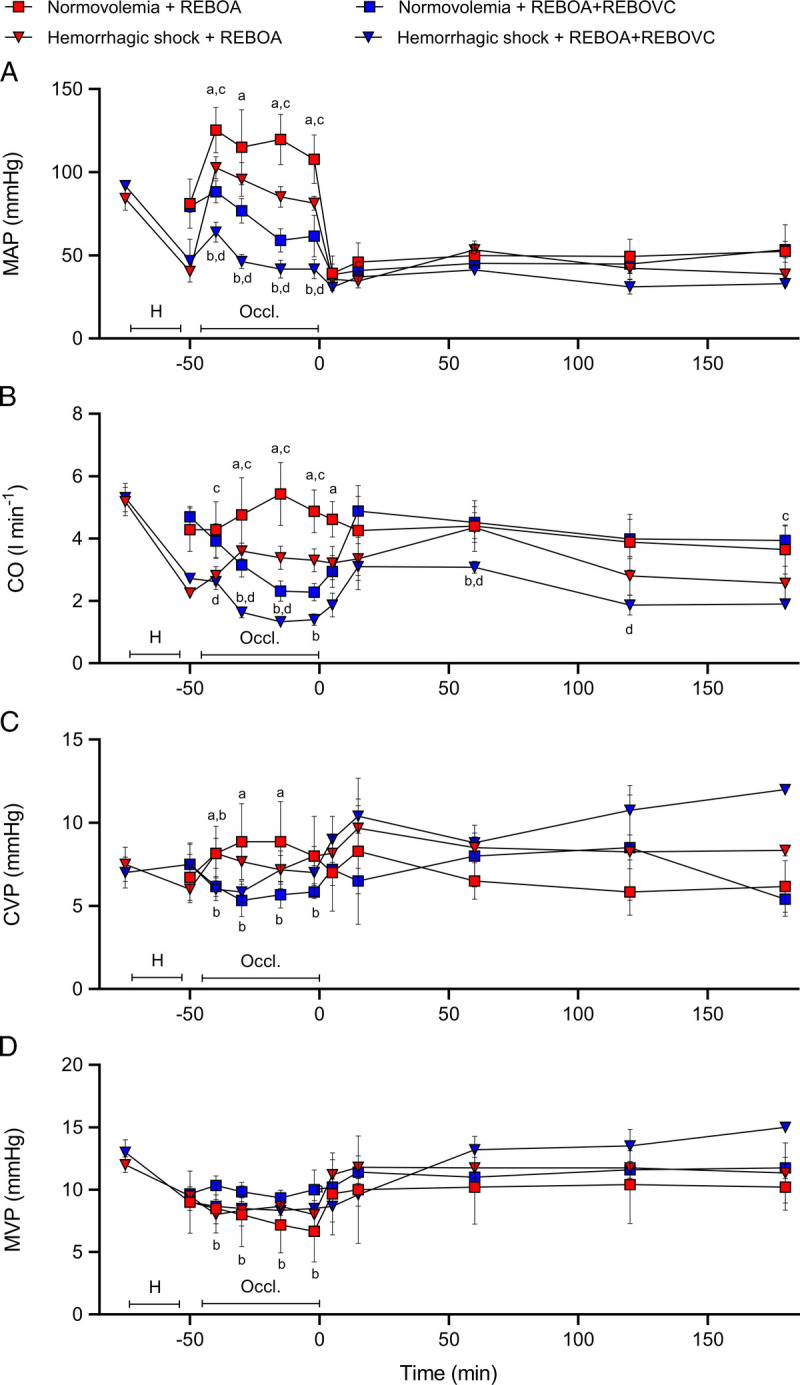
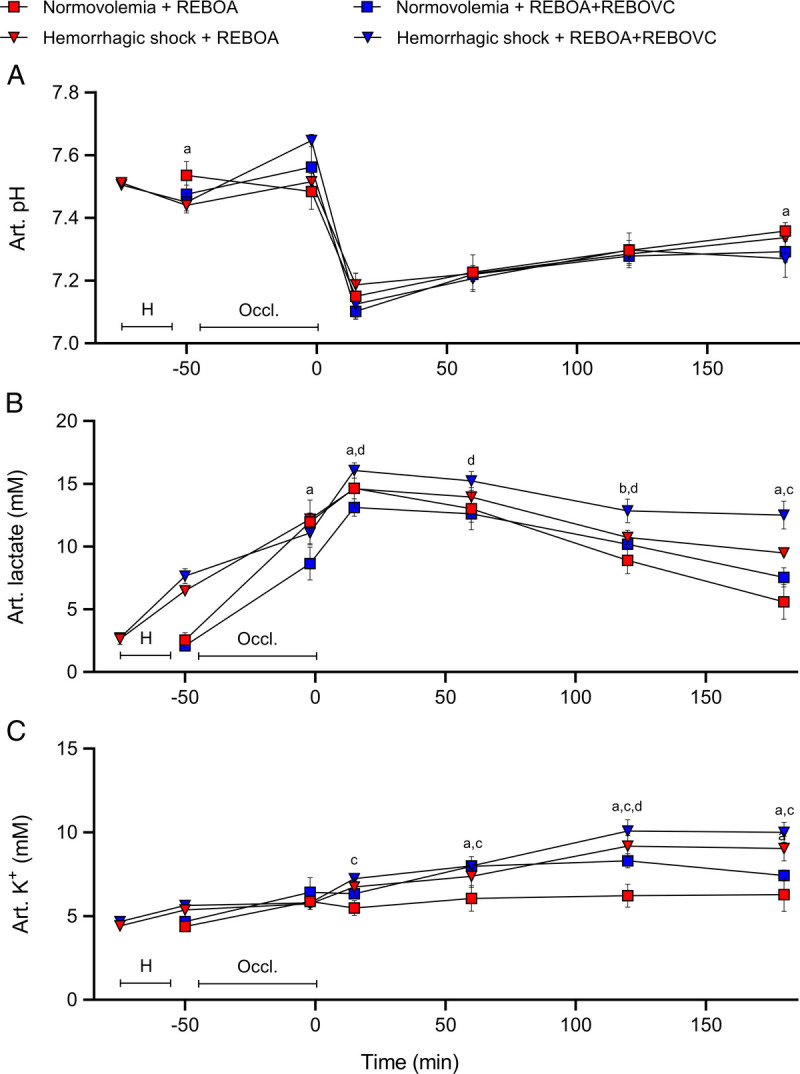
Results: During occlusion, both the REBOA groups had higher systemic mean arterial pressure (MAP) and cardiac output (p < 0.05) compared with the two REBOA+REBOVC groups. After 60 minutes reperfusion, there were no statistically significant differences between the two REBOA groups and the two REBOA+REBOVC groups in MAP and cardiac output. The two REBOA+REBOVC groups had higher arterial lactate and potassium concentrations during reperfusion, compared with the two REBOA groups (p < 0.05). There was no major difference in end-organ damage markers between REBOA and REBOA+REBOVC. Survival after 1-hour reperfusion was 86% and 100%, respectively, in the normovolemic REBOA and REBOA+REBOVC groups, and 67% and 83%, respectively, in the corresponding hemorrhagic shock REBOA and REBOA+REBOVC groups.
Conclusion: Acceptable hemodynamic stability during occlusion and short-term survival can be achieved by REBOA+REBOVC with adequate resuscitation; however, the more severe hemodynamic and metabolic impacts of REBOA+REBOVC compared with REBOA must be considered.
Level of evidence: Prospective, randomized, experimental animal study. Basic science study, therapeutic.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Surgery of Trauma.
Figures
References
-
- Ciresi KF, Lim RC, Jr. Hepatic vein and retrohepatic vena caval injury. World J Surg. 1990;14(4):472–477. - PubMed
-
- Buechter KJ, Sereda D, Gomez G, Zeppa R. Retrohepatic vein injuries: experience with 20 cases. J Trauma. 1989;29(12):1698–1704. - PubMed
-
- Khaneja SC, Pizzi WF, Barie PS, Ahmed N. Management of penetrating juxtahepatic inferior vena cava injuries under total vascular occlusion. J Am Coll Surg. 1997;184(5):469–474. - PubMed
-
- Millikan JS, Moore EE, Cogbill TH, Kashuk JL. Inferior vena cava injuries–a continuing challenge. J Trauma. 1983;23(3):207–212. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
