

Comorbidities and healthcare costs and resource use of patients with nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) in the Japan medical data vision database
- PMID: 33496858
- PMCID: PMC7932941
- DOI: 10.1007/s00535-021-01759-2
Comorbidities and healthcare costs and resource use of patients with nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) in the Japan medical data vision database
Abstract
Background: This study examined demographics, comorbidities and healthcare resource use (HCRU) and costs among Japanese patients with nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH).
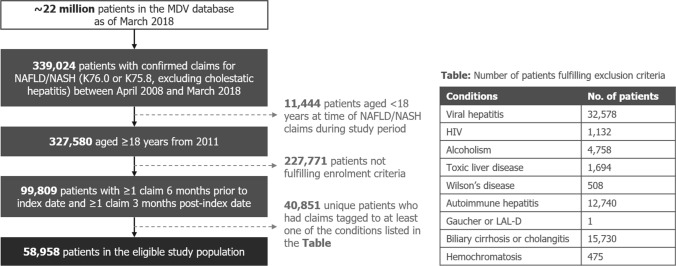
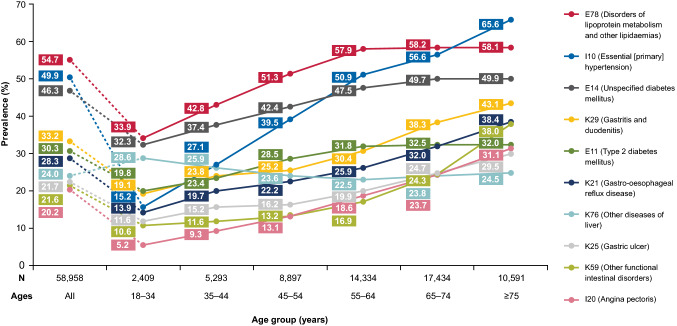
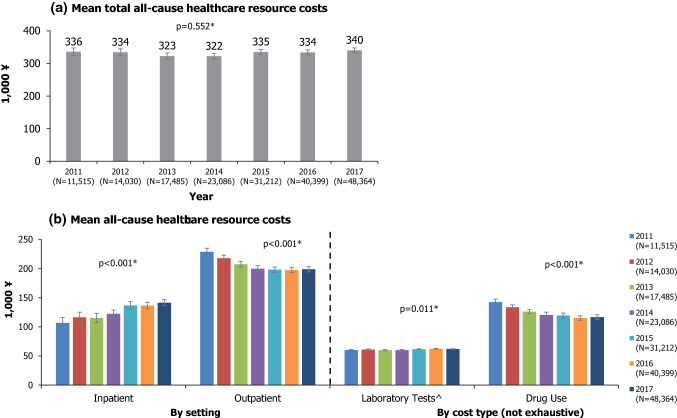
Methods: We conducted a repeated cross-sectional analysis of the Medical Data Vision (MDV) claims database, from January 2011 to March 2018. Demographics were described at index date and by calendar year; a "NASH" subpopulation included patients with ≥ 1 claim for NASH at any time. Prevalence of pre-specified comorbidities of interest and data-emergent top comorbidities were estimated. All-cause HCRU and costs were quantified by calendar year. Outcomes were compared between 2011 and 2017 using partially overlapping t tests.
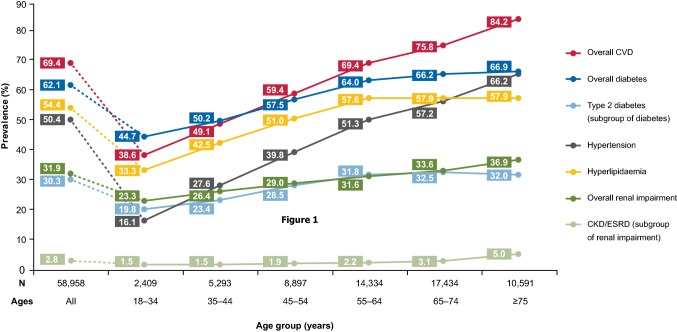
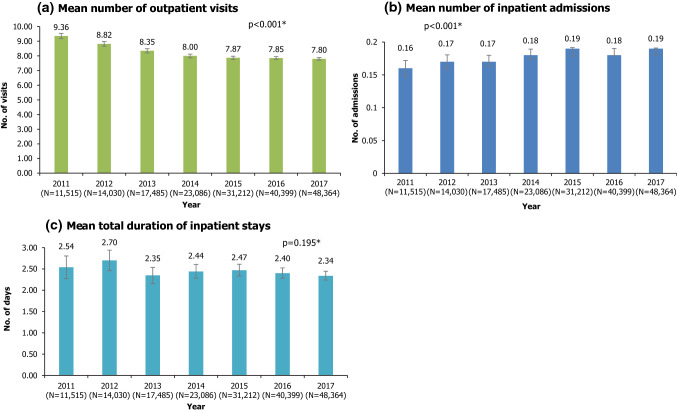
Results: 58,958 patients (mean age 61.6 years; 55.5% male) were included. 1139 patients (2%) were in the NASH subpopulation. At baseline, comorbid cardiovascular disease (69.4%), diabetes (62.1%) and hyperlipidaemia (54.4%) were most prevalent; comorbidity prevalence increased with age. Mean outpatient visits decreased from 9.36 per patient in 2011 to 7.80 in 2017; mean inpatient admissions increased (both p < 0.001 for 2011 vs 2017). Mean total all-cause healthcare costs ranged from ¥322,206 to ¥340,399 per patient per year between 2011 and 2017. Although total all-cause healthcare costs did not change significantly (p = 0.552), cost burden shifted from the outpatient to inpatient setting between 2011 and 2017. All-cause healthcare resource use/costs were generally higher for the NASH subgroup compared with the overall population.
Conclusions: There is a high burden of disease among Japanese NAFLD/NASH patients, including a high prevalence of comorbidities which generally increase with age. Accordingly, substantial all-cause HCRU and costs were incurred.
Keywords: Cost; Database analysis; Japan; Nonalcoholic fatty liver disease; Nonalcoholic steatohepatitis.
Conflict of interest statement
Amy Buchanan-Hughes and Alvin Ng are employees of Costello Medical, which was funded by Gilead Sciences to provide data analysis, research, writing and editorial services for this manuscript. I-Heng Lee and Ken Hasegawa are employees of Gilead Sciences. Shuji Terai has no conflicts of interests to declare.
Figures
References
-
- Fan J-G, Kim S-U, Wong VW-S. New trends on obesity and NAFLD in Asia. J Hepatol. 2017;67:862–73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
