

Exploring and Overcoming the Challenges Primary Care Practices Face with Care Management of High-Risk Patients in CPC+: a Mixed-Methods Study
- PMID: 33496929
- PMCID: PMC8481356
- DOI: 10.1007/s11606-020-06528-0
Exploring and Overcoming the Challenges Primary Care Practices Face with Care Management of High-Risk Patients in CPC+: a Mixed-Methods Study
Abstract
Background: Longitudinal care management (LCM) for high-risk patients is a cornerstone of primary care models aiming to improve quality and reduce costs.
Objective: Describe the extent to which LCM was implemented in the second year of Comprehensive Primary Care Plus (CPC+), and barriers to and facilitators of implementation.
Design: Mixed-methods.
Participants: Quantitative: 2715 practices participating in CPC+ in 2018. Qualitative: Interviews with practitioners and staff in 23 representative CPC+ practices.
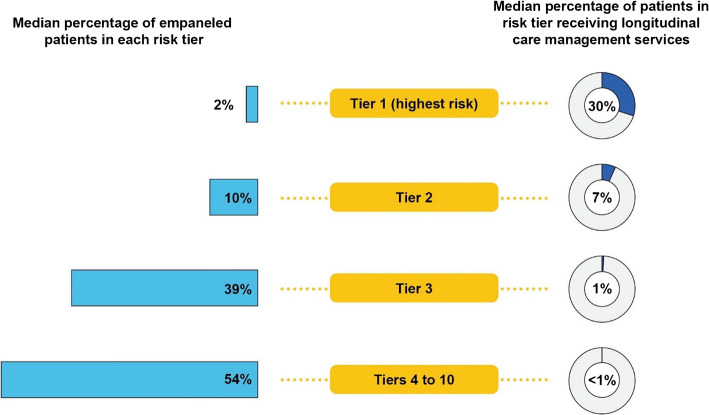
Main measures: Across all CPC+ practices, we report median percentages of empaneled patients placed in the highest-risk tiers and, of those, the median percentage receiving LCM. Across 23 CPC+ practices, we report qualitative findings on LCM implementation.
Key results: While practices reported benefits of LCM, a small proportion of patients received LCM. Practices placed 2.4% (median) of patients in the highest-risk tier; of these, 30% (median) received LCM. Practices placed 10% (median) of patients in the second-highest-risk tier; of these, 7% (median) received LCM. Interviews revealed LCM uptake across tiers was low because of insufficient care manager staffing. Other challenges included lack of practitioner buy-in to using risk stratification to identify high-risk patients, patients' reluctance to engage in LCM or change behaviors, and limited health information technology functionality for developing, maintaining, and accessing high-risk patients' care plans. Facilitators included embedding care managers within practices and electronic health record functionalities that support LCM.
Conclusions: Despite substantial financial and other supports, and practices' perceived benefits of LCM, insufficient care manager staffing and other barriers have limited its potential in CPC+ to date. To expand LCM's reach, practices need additional care managers, training to overcome barriers to patient engagement, better identification of patients who might benefit from LCM, improved information technology tools for risk stratification and care plans, and more practitioner buy-in to risk stratification.
Keywords: care management; care plans; high-risk patients; primary health care; risk stratification.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Peikes D, Anglin G, Harrington M, et al. Independent evaluation of Comprehensive Primary Care Plus (CPC+): first annual report. Princeton (NJ): Mathematica; 2019 April. Contract No: HHSM-500-2014-000341/HHSM-500-T0010. Sponsored by the U.S. Department of Health and Human Services, Center for Medicare & Medicaid Innovation.
-
- Anglin G, Peikes D, Petersen D, et al. Independent evaluation of Comprehensive Primary Care Plus (CPC+): second annual report. Princeton (NJ): Mathematica; 2020 July. Contract No: HHSM-500-2014-00341/HHSM-500-T0010. Sponsored by the U.S. Department of Health and Human Services, Center for Medicare & Medicaid Innovation.
-
- Centers for Medicare & Medicaid Services. 2018 CPC+ implementation guide: guiding principles and reporting. Washington, DC: CMS, January 30, 2018.
-
- Berry-Millet R, Bodenheimer TS. Care management of patients with complex health care needs. Synth Proj Synth Rep. 2009;19:52372. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
