

Therapeutic Options for Recurrence of Primary Focal Segmental Glomerulonephritis (FSGS) in the Renal Allograft: Single-Center Experience
- PMID: 33498160
- PMCID: PMC7863737
- DOI: 10.3390/jcm10030373
Therapeutic Options for Recurrence of Primary Focal Segmental Glomerulonephritis (FSGS) in the Renal Allograft: Single-Center Experience
Abstract
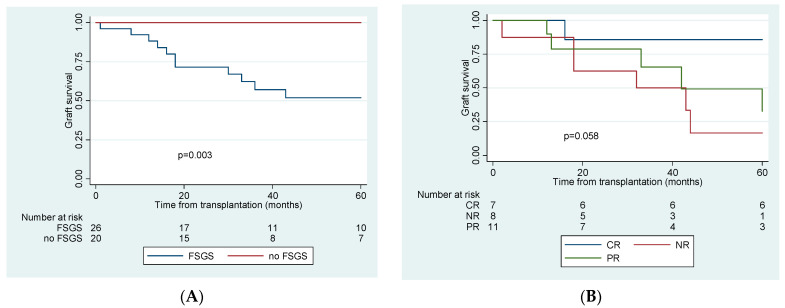
Focal Segmental Glomerulosclerosis (FSGS) recurrence after kidney transplantation (KTx) is relatively frequent and is associated with poor graft survival. The aim of this study was to investigate which management strategies were associated with better outcomes in our cohort of KTx recipients with primary FSGS. We retrospectively collected data on patients with primary FSGS who received a KTx between 1993 and 2019. A history of biopsy proven FSGS in native kidneys and new onset of significant proteinuria early post-KTx led to the diagnosis of recurrence, which was confirmed by graft biopsy. From 1993 to 2019 we performed 46 KTxs in patients with primary FSGS. We identified 26 episodes of recurrence in 25 patients, 67% of them occurring in males. They were younger at the time of KTx (33.8 vs. 41.1 years old, p = 0.067) and had progressed to end stage renal disease (ESRD) faster after FSGS diagnosis (61.4 vs. 111.2 months, p = 0.038), while they were less likely to have received prophylactic plasmapheresis (61.5% vs. 90%, p = 0.029). 76.7% of recurrences were found early, after a median of 0.5 months (IQR 0.1-1) with a median proteinuria was 8.5 (IQR 4.9-11.9) g/day. All patients with recurrence were treated with plasmapheresis, while 8 (30.7%) additionally received rituximab, 1 (3.8%) abatacept, and 4 (15.4%) ACTH. 7 (27%) patients experienced complete and 11 (42.3%) partial remission after a mean time of 3 (±1.79) and 4.4 (±2.25) months, respectively. Prognosis was worse for patients who experienced a recurrence. Eleven (42.3%) patients lost their graft from FSGS in a median time of 33 (IQR 17.5-43.3) months. In this series of patients, primary FSGS recurred frequently after KTx. Prophylacic plasmapheresis was shown efficacious in avoiding FSGS recurrence, while timely diagnosis and plasmapheresis-based regimens induced remission in more than half of the patients.
Keywords: FSGS recurrence; kidney transplantation; outcomes; plasmapheresis; therapeutic agents.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Schena F.P. Epidemiology of end-stage renal disease: International comparisons of renal replacement therapy. Kidney Int. 2000;57:S39–S45. doi: 10.1046/j.1523-1755.2000.07407.x. - DOI
-
- Hickson L.J., Gera M., Amer H., Iqbal C.W., Moore T.B., Milliner D.S., Cosio F.G., Larson T.S., Stegall M.D., Ishitani M.B., et al. Kidney Transplantation for Primary Focal Segmental Glomerulosclerosis: Outcomes and Response to Therapy for Recurrence. Transplantation. 2009;87:1232–1239. doi: 10.1097/TP.0b013e31819f12be. - DOI - PubMed
-
- Uffing A., Pérez-Sáez M.J., Mazzali M., Manfro R.C., Bauer A.C., de SottomaiorDrumond F., O’shaughnessy M.M., Cheng X.S., Chin K.K., Ventura C.G., et al. Recurrence of FSGS after Kidney Transplantation in Adults. Clin. J. Am. Soc. Nephrol. 2020;15:247. doi: 10.2215/CJN.08970719. - DOI - PMC - PubMed
-
- Maas R.J.H., Deegens J.K.J., van den Brand J.A.J.G., Cornelissen E.A.M., Wetzels J.F.M. A retrospective study of focal segmental glomerulosclerosis: Clinical criteria can identify patients at high risk for recurrent disease after first renal transplantation. BMC Nephrol. 2013;14:47. doi: 10.1186/1471-2369-14-47. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
