

Validation of Prognostic Scores in Extracorporeal Life Support: A Multi-Centric Retrospective Study
- PMID: 33498825
- PMCID: PMC7912316
- DOI: 10.3390/membranes11020084
Validation of Prognostic Scores in Extracorporeal Life Support: A Multi-Centric Retrospective Study
Abstract
Multiple prognostic scores have been developed for both veno-arterial (VA) and veno-venous (VV) extracorporeal membrane oxygenation (ECMO), mostly in single-center cohorts. The aim of this study was to compare and validate different prediction scores in a large multicenter ECMO-population.
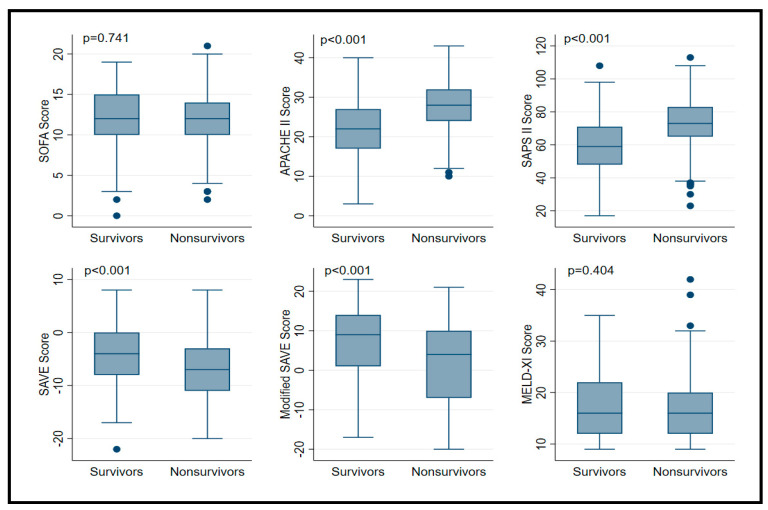
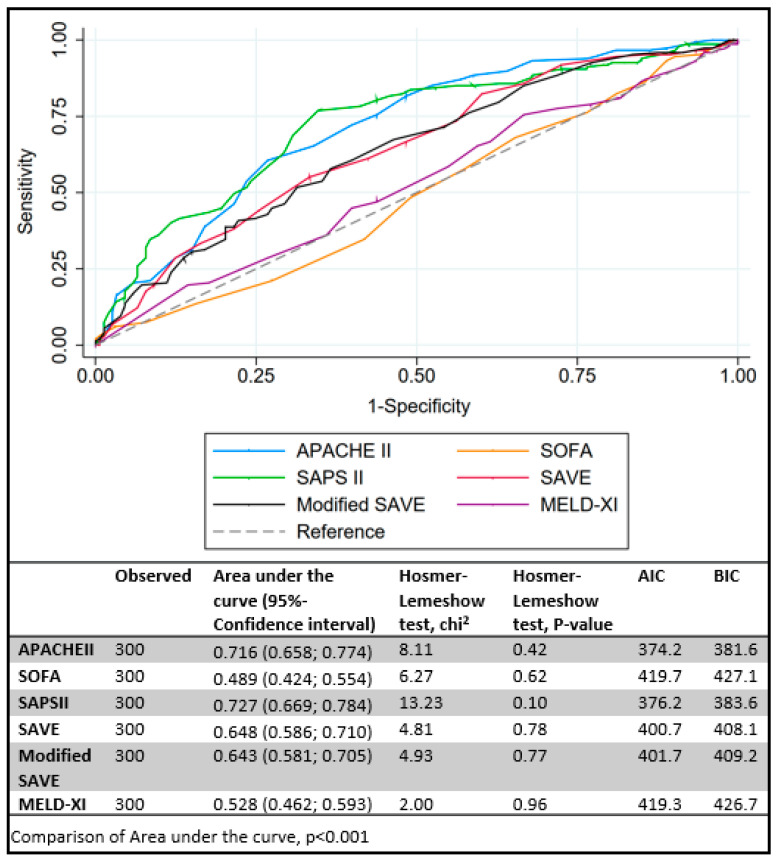
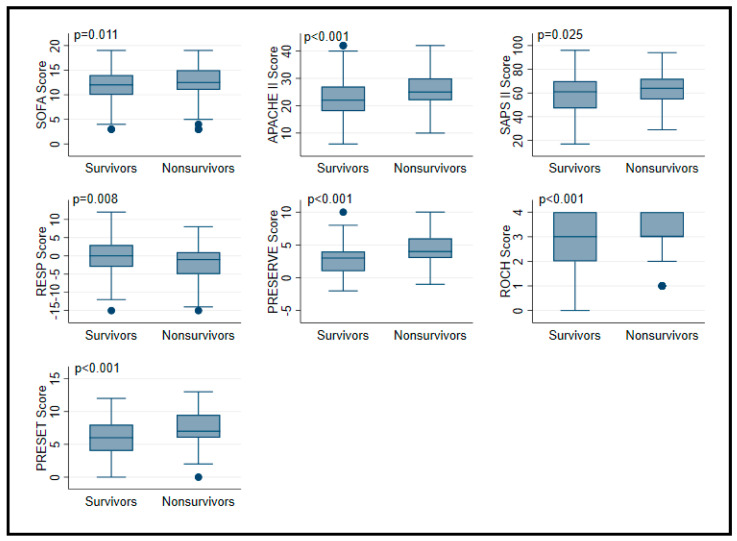
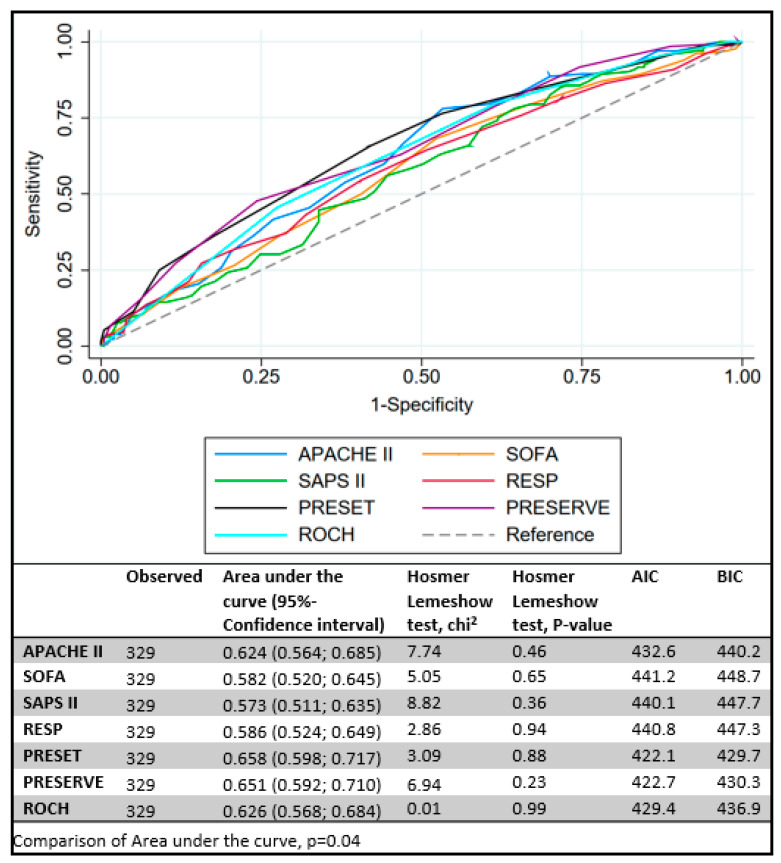
Methods: Data from five ECMO centers included 300 patients on VA and 329 on VV ECMO support (March 2008 to November 2016). Different prognostic scores were compared between survivors and non-survivors: APACHE II, SOFA, SAPS II in all patients; SAVE, modified SAVE and MELD-XI in VA ECMO; RESP, PRESET, ROCH and PRESERVE in VV ECMO. Model performance was compared using receiver-operating-curve analysis and assessment of model calibration. Survival was assessed at intensive care unit discharge.
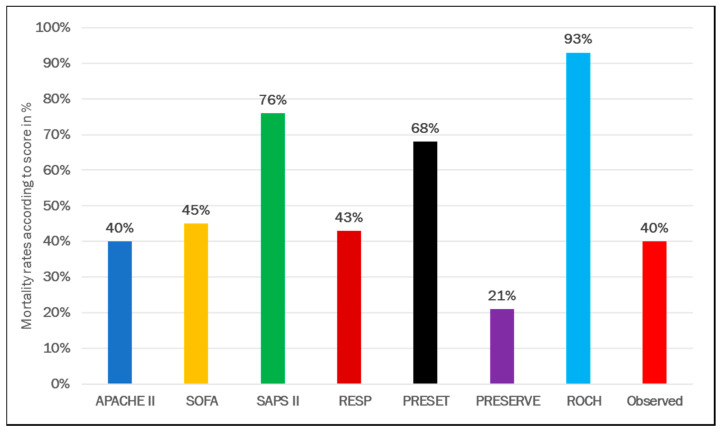
Results: The main indication for VA ECMO was cardiogenic shock; overall survival was 51%. ICU survivors had higher Glasgow Coma Scale scores and pH, required cardiopulmonary resuscitation (CPR) less frequently, had lower lactate levels and shorter ventilation time pre-ECMO at baseline. The best discrimination between survivors and non-survivors was observed with the SAPS II score (area under the curve [AUC] of 0.73 (95% CI 0.67-0.78)). The main indication for VV ECMO was pneumonia; overall survival was 60%. Lower PaCO2, higher pH, lower lactate and lesser need for CPR were observed among survivors. The best discrimination between survivors and non-survivors was observed with the PRESET score (AUC 0.66 (95% CI 0.60-0.72)).
Conclusion: The prognostic performance of most scores was moderate in ECMO patients. The use of such scores to decide about ECMO implementation in potential candidates should be discouraged.
Keywords: ECLS; ECMO; RESP score; SAVE score; score; validation.
Conflict of interest statement
F.S.T., L.M.B., M.B., F.P. and M.V.M. received consultancy fees from Eurosets (Medolla, Italy), M.B. received fees as a congress speaker from Hamilton Medical (Bonaduz, Swiss), L.M.B. received consultancy fees from Xenios AG (Heilbronn, Germany). All other authors have no conflicts of interests to declare.
Figures
References
-
- Brogan T.V., Lequier L., Lorusso R., MacLaren G., Peek G.J. The ELSO Red Book. 5th ed. Extracorporeal Life Support Organization; Ann Arbor, MI, USA: 2017. Extracorporeal life support.
-
- Schmidt M., Burrell A., Roberts L., Bailey M., Sheldrake J., Rycus P.T., Hodgson C., Scheinkestel C., Cooper D.J., Thiagarajan R.R., et al. Predicting survival after ECMO for refractory cardiogenic shock: The survival after veno-arterial-ECMO (SAVE)-score. Eur. Heart J. 2015;36:2246–2256. doi: 10.1093/eurheartj/ehv194. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
