

Linking Labile Heme with Thrombosis
- PMID: 33499296
- PMCID: PMC7865584
- DOI: 10.3390/jcm10030427
Linking Labile Heme with Thrombosis
Abstract
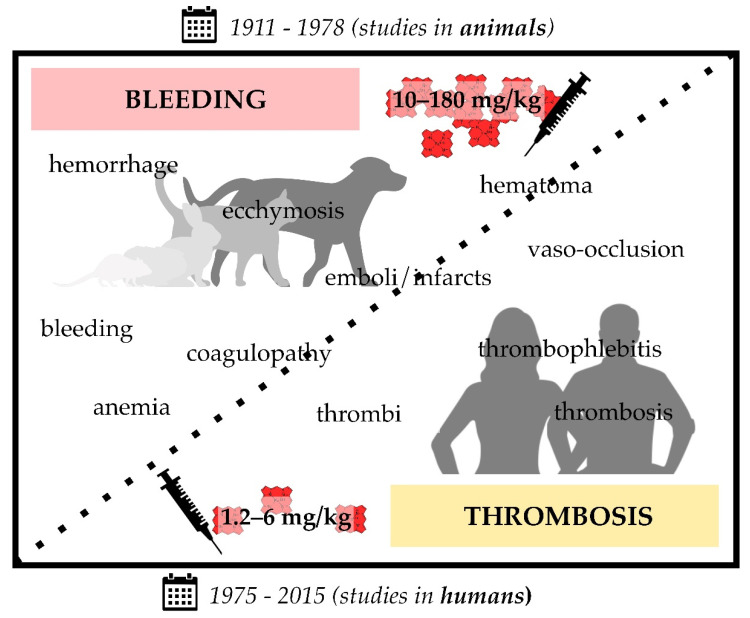
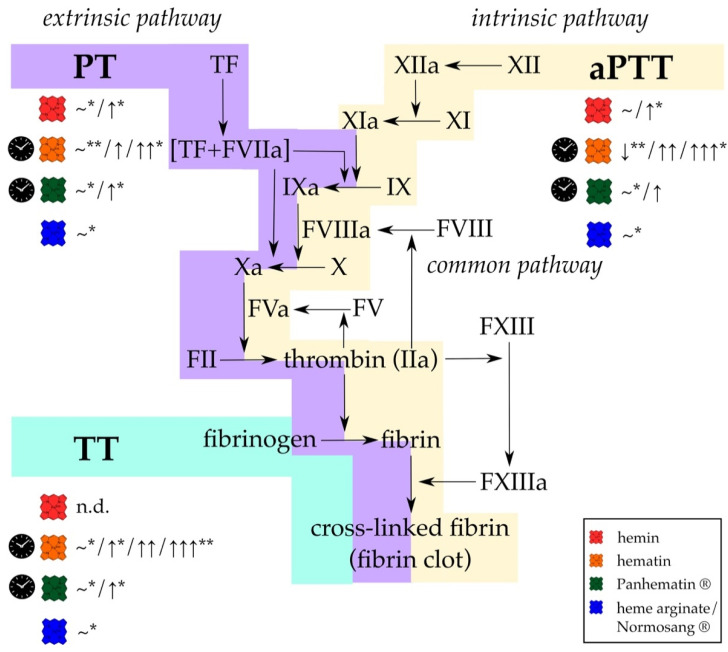
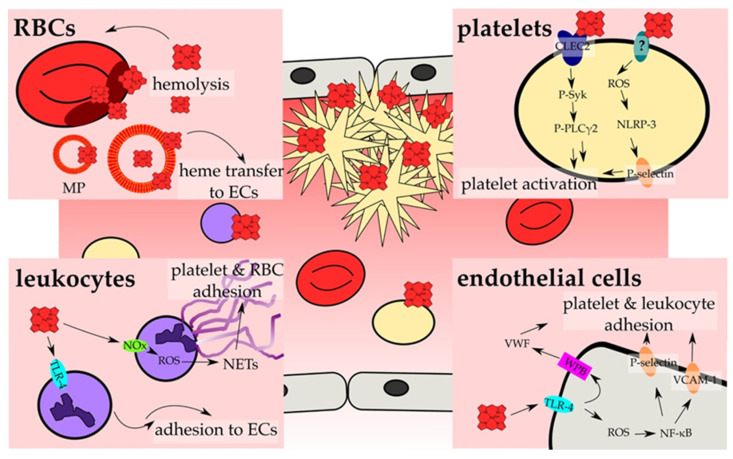
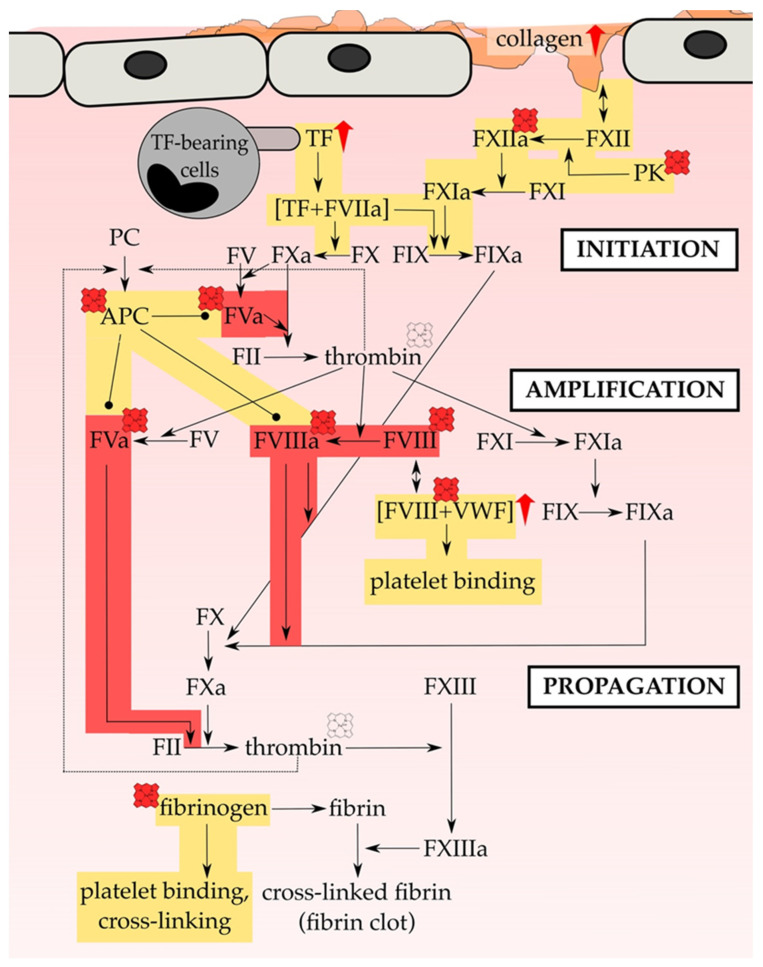
Thrombosis is one of the leading causes of death worldwide. As such, it also occurs as one of the major complications in hemolytic diseases, like hemolytic uremic syndrome, hemorrhage and sickle cell disease. Under these conditions, red blood cell lysis finally leads to the release of large amounts of labile heme into the vascular compartment. This, in turn, can trigger oxidative stress and proinflammatory reactions. Moreover, the heme-induced activation of the blood coagulation system was suggested as a mechanism for the initiation of thrombotic events under hemolytic conditions. Studies of heme infusion and subsequent thrombotic reactions support this assumption. Furthermore, several direct effects of heme on different cellular and protein components of the blood coagulation system were reported. However, these effects are controversially discussed or not yet fully understood. This review summarizes the existing reports on heme and its interference in coagulation processes, emphasizing the relevance of considering heme in the context of the treatment of thrombosis in patients with hemolytic disorders.
Keywords: blood coagulation; coagulation factors; heme binding; hemolysis; hemolytic diseases; hemorrhage; labile heme; platelets; thrombosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
