

Hospital bed capacity and usage across secondary healthcare providers in England during the first wave of the COVID-19 pandemic: a descriptive analysis
- PMID: 33500288
- PMCID: PMC7843315
- DOI: 10.1136/bmjopen-2020-042945
Hospital bed capacity and usage across secondary healthcare providers in England during the first wave of the COVID-19 pandemic: a descriptive analysis
Abstract
Objective: In this study, we describe the pattern of bed occupancy across England during the peak of the first wave of the COVID-19 pandemic.
Design: Descriptive survey.
Setting: All non-specialist secondary care providers in England from 27 March27to 5 June 2020.
Participants: Acute (non-specialist) trusts with a type 1 (ie, 24 hours/day, consultant-led) accident and emergency department (n=125), Nightingale (field) hospitals (n=7) and independent sector secondary care providers (n=195).
Main outcome measures: Two thresholds for 'safe occupancy' were used: 85% as per the Royal College of Emergency Medicine and 92% as per NHS Improvement.
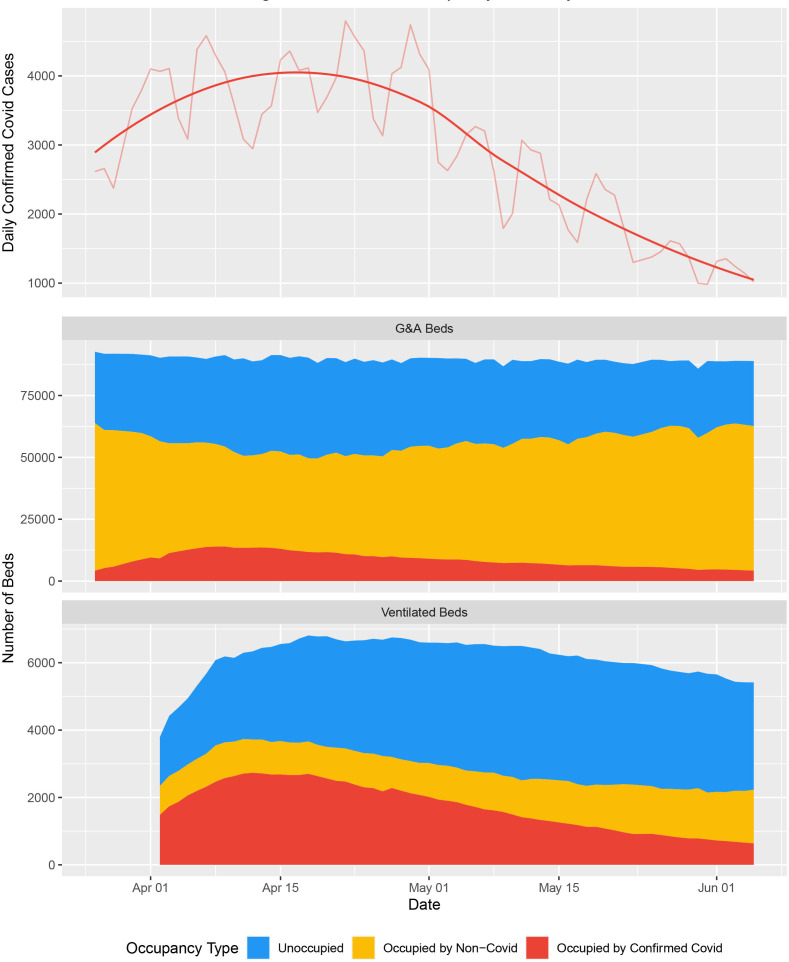
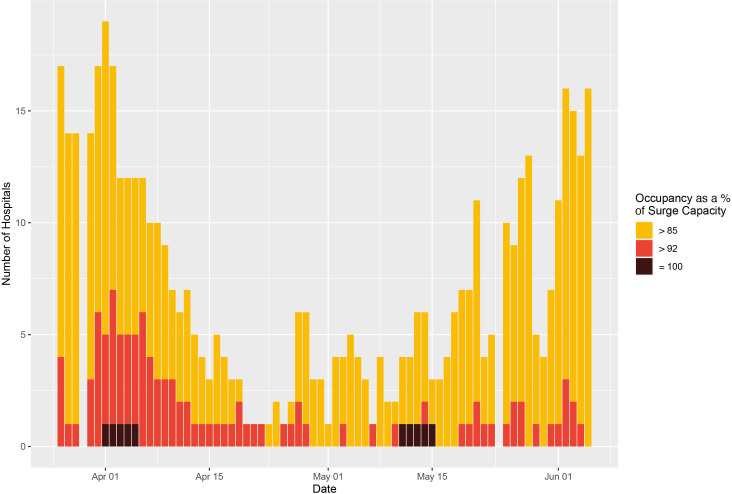
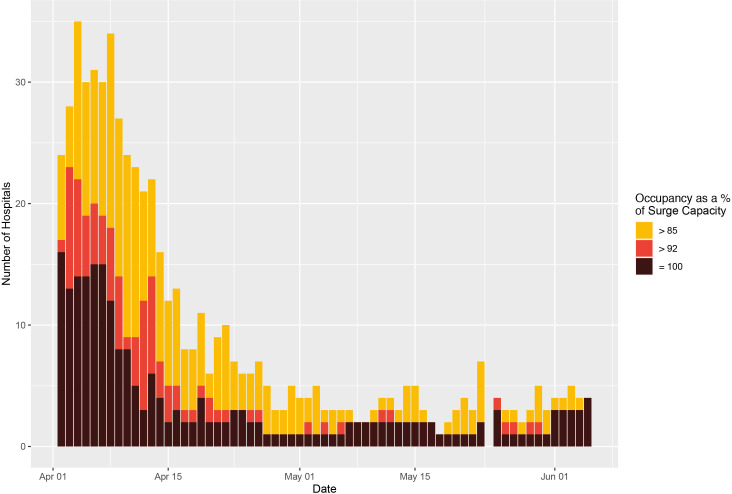
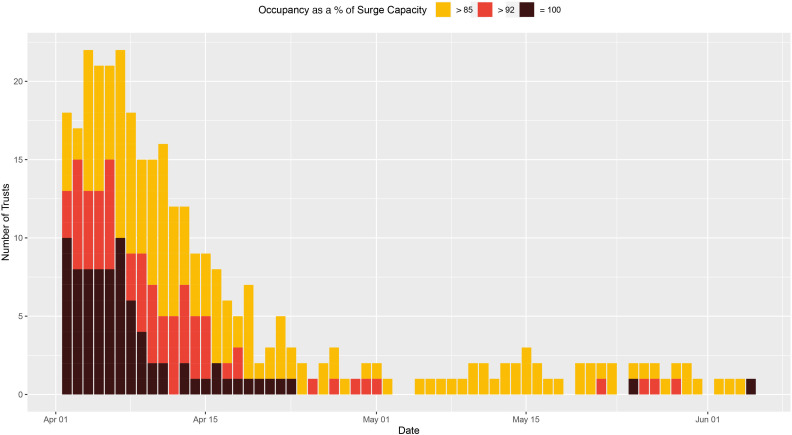
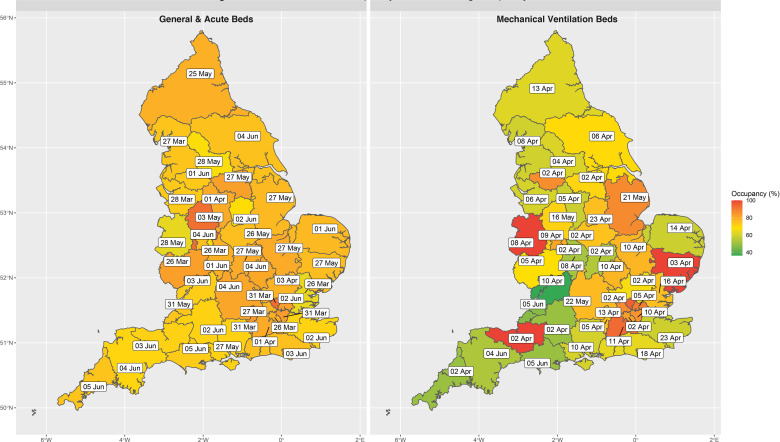
Results: At peak availability, there were 2711 additional beds compatible with mechanical ventilation across England, reflecting a 53% increase in capacity, and occupancy never exceeded 62%. A consequence of the repurposing of beds meant that at the trough there were 8.7% (8508) fewer general and acute beds across England, but occupancy never exceeded 72%. The closest to full occupancy of general and acute bed (surge) capacity that any trust in England reached was 99.8% . For beds compatible with mechanical ventilation there were 326 trust-days (3.7%) spent above 85% of surge capacity and 154 trust-days (1.8%) spent above 92%. 23 trusts spent a cumulative 81 days at 100% saturation of their surge ventilator bed capacity (median number of days per trust=1, range: 1-17). However, only three sustainability and transformation partnerships (aggregates of geographically co-located trusts) reached 100% saturation of their mechanical ventilation beds.
Conclusions: Throughout the first wave of the pandemic, an adequate supply of all bed types existed at a national level. However, due to an unequal distribution of bed utilisation, many trusts spent a significant period operating above 'safe-occupancy' thresholds despite substantial capacity in geographically co-located trusts, a key operational issue to address in preparing for future waves.
Keywords: COVID-19; health policy; intensive & critical care; public health.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: AM declares previous research funding from Eli Lilly and Company, Pfizer and AstraZeneca. SV declares funding from IQVIA. All other authors declare no competing interests.
Figures
References
-
- The King’s Fund NHS Hospital bed numbers, 2020. Available: https://www.kingsfund.org.uk/publications/nhs-hospital-bed-numbers [Accessed 21 June 2020].
-
- The Health Foundation The NHS this winter: looking beneath the National view | the health Foundation. Available: https://www.health.org.uk/news-and-comment/blogs/the-nhs-this-winter-loo... [Accessed 21 Jun 2020].
-
- British Medical Association Bed occupancy in the NHS - Pressures - BMA. The British Medical Association is the trade union and professional body for doctors in the UK, 2020. Available: https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/pre... [Accessed 21 Jun 2020].
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical