

Chemotherapy-induced changes in tumor consistency can allow gross total resection of previously unresectable brainstem pilocytic astrocytoma
- PMID: 33500827
- PMCID: PMC7827363
- DOI: 10.25259/SNI_594_2020
Chemotherapy-induced changes in tumor consistency can allow gross total resection of previously unresectable brainstem pilocytic astrocytoma
Abstract
Background: Low-grade gliomas (LGG) are described by the World Health Organization as Grades I and II. Among LGGs, the most common primary brain tumor is pilocytic astrocytoma (PA) and carries an excellent prognosis when treated with complete surgical resection. Cases, in which this is not possible, are associated with less favorable outcomes and worse progression-free survival.
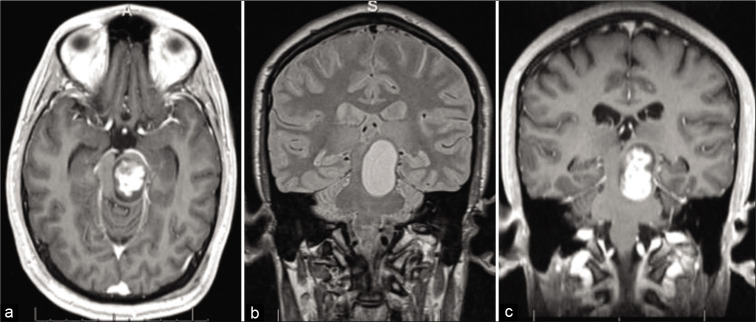
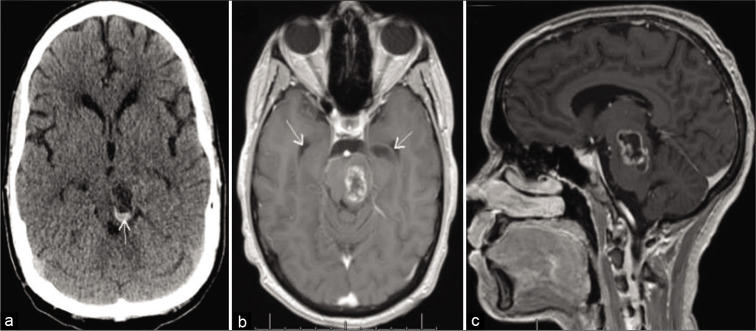
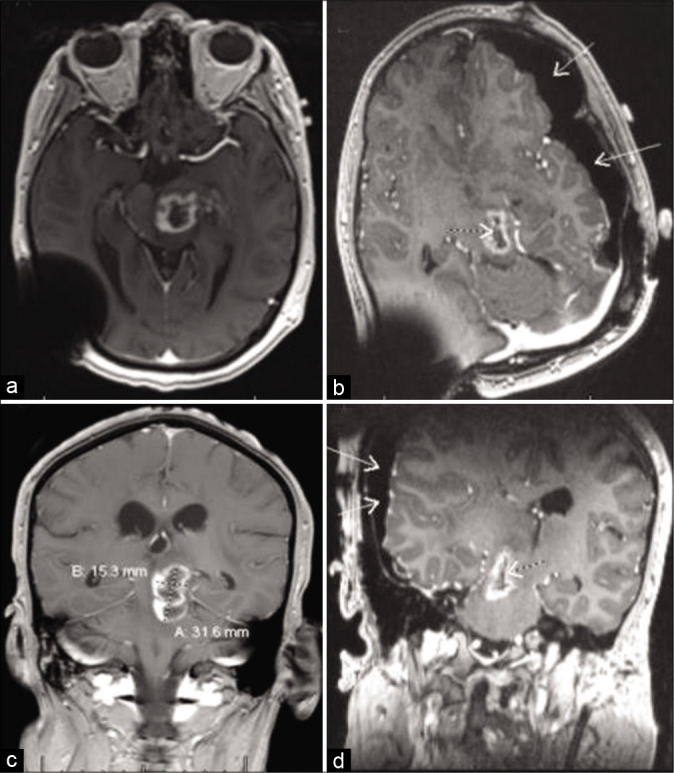
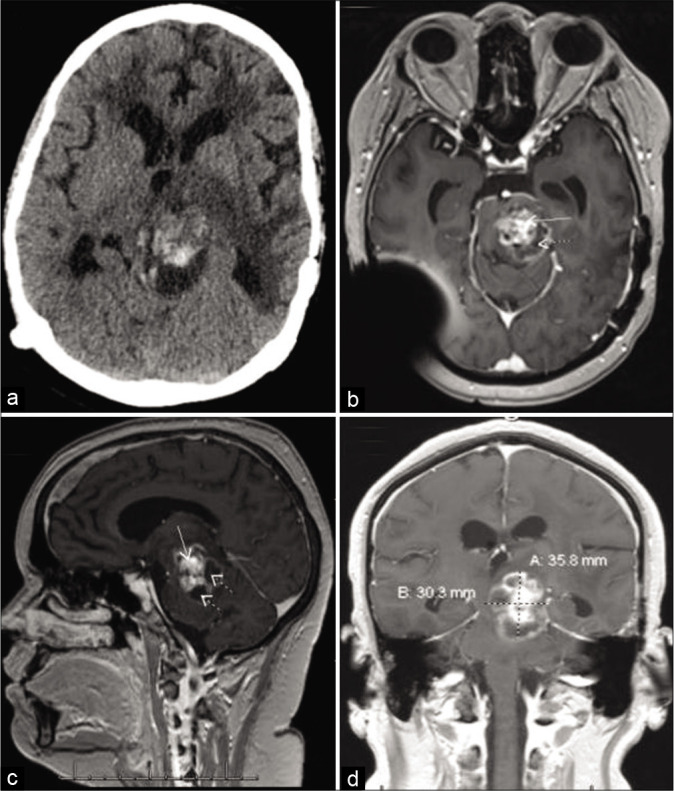
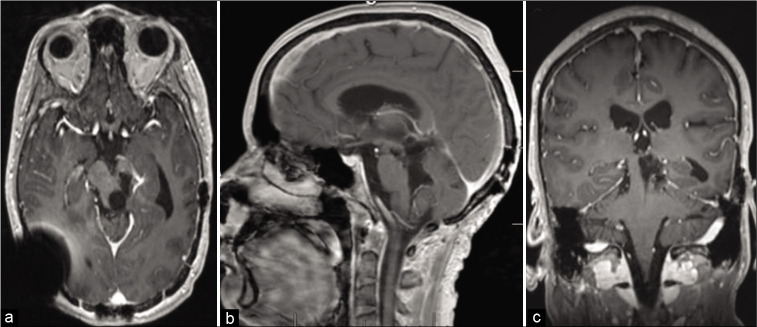
Case description: This report describes a case of a 22-year-old male, who presented with progression of a primary brainstem tumor previously treated with stereotactic radiosurgery and chemotherapy. Patient underwent surgical exploration and was diagnosed with juvenile PA, but debulking was limited by the very dense and fibrous tumor. Complete surgical resection was not possible at this time. Despite efforts to treat with chemotherapy, the patient presented a year later with clinical deterioration and severe neurologic deficits, prompting surgical re-exploration. During the second operation, the tumor was found to have undergone very significant softening in consistency, allowing for gross total resection (GTR).
Conclusion: Aggressive treatment of brainstem LGG should be pursued whenever possible, given its generally favorable prognosis. Repeat microsurgical resection, even with a different approach, might be reasonable and safe. Finally, chemotherapy may be associated with changes in the tumor consistency that can render previously unresectable lesions amenable to successful aggressive resection.
Keywords: Brainstem low-grade glioma; Chemotherapy; Gross total resection; Pilocytic astrocytoma; Tumor consistency.
Copyright: © 2020 Surgical Neurology International.
Conflict of interest statement
There are no conflicts of interest.
Figures
Similar articles
-
Proposed therapeutic strategy for adult low-grade glioma based on aggressive tumor resection.Neurosurg Focus. 2015 Jan;38(1):E7. doi: 10.3171/2014.10.FOCUS14651. Neurosurg Focus. 2015. PMID: 25599276
-
Results of a policy of surveillance alone after surgical management of pediatric low grade gliomas.Int J Radiat Oncol Biol Phys. 2001 Nov 1;51(3):704-10. doi: 10.1016/s0360-3016(01)01705-9. Int J Radiat Oncol Biol Phys. 2001. PMID: 11597812
-
Twenty-three years follow-up after low-dose Gamma Knife surgery of a brainstem juvenile pilocytic astrocytoma: a case report and review of the literature.Childs Nerv Syst. 2019 Jul;35(7):1227-1230. doi: 10.1007/s00381-019-04147-7. Epub 2019 Apr 17. Childs Nerv Syst. 2019. PMID: 30997566 Review.
-
Intra-axial tumors of the cervicomedullary junction: surgical results and long-term outcome.Pediatr Neurosurg. 1997 Jul;27(1):12-8. doi: 10.1159/000121219. Pediatr Neurosurg. 1997. PMID: 9486831
-
Successful Surgery of Exophytic Brainstem Glioma Mimicking Cerebellar-Pontine Angle Tumor: Case Report and Review of Literature.World Neurosurg. 2019 Aug;128:202-205. doi: 10.1016/j.wneu.2019.05.053. Epub 2019 May 14. World Neurosurg. 2019. PMID: 31100526 Review.
References
-
- Burkhard C, di Patre PL, Schüler D, Schüler G, Yaşargil NG, Yonekawa Y, et al. A population-based study of the incidence and survival rates in patients with pilocytic astrocytoma. J Neurosurg. 2003;98:1170–4. - PubMed
-
- Gagliardi F, Bailo M, Spina A, Donofrio CA, Boari N, Franzin A, et al. Gamma knife radiosurgery for low-grade gliomas: Clinical results at long-term follow-up of tumor control and patients quality of life. World Neurosurg. 2017;101:540–53. - PubMed
-
- Kestle J, Townsend JJ, Brockmeyer DL, Walker M. Juvenile pilocytic astrocytoma of the brainstem in children. J Neurosurg. 2004;101(Suppl 1):1–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources