

Monocytes carrying GFAP detect glioma, brain metastasis and ischaemic stroke, and predict glioblastoma survival
- PMID: 33501422
- PMCID: PMC7811761
- DOI: 10.1093/braincomms/fcaa215
Monocytes carrying GFAP detect glioma, brain metastasis and ischaemic stroke, and predict glioblastoma survival
Abstract
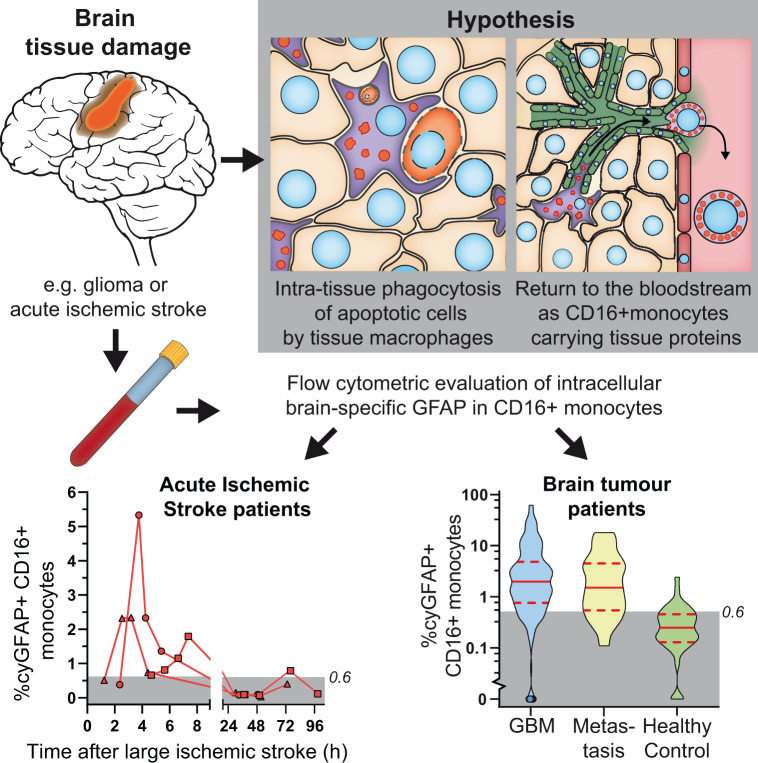
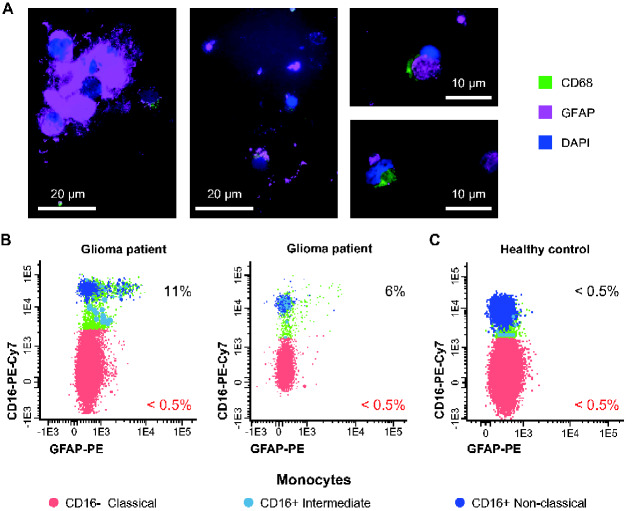
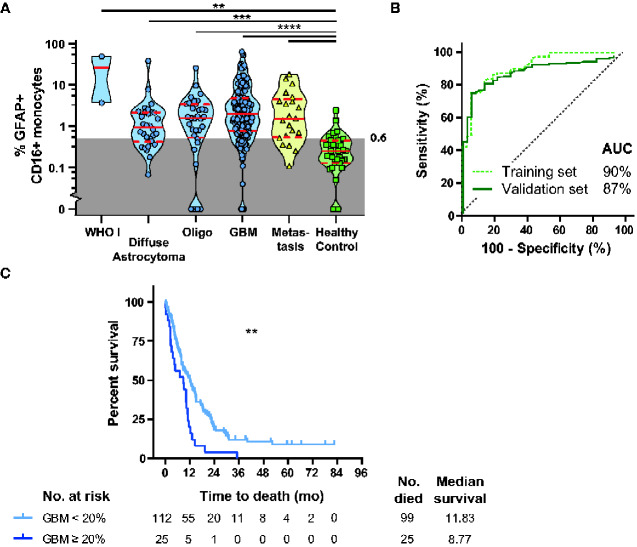
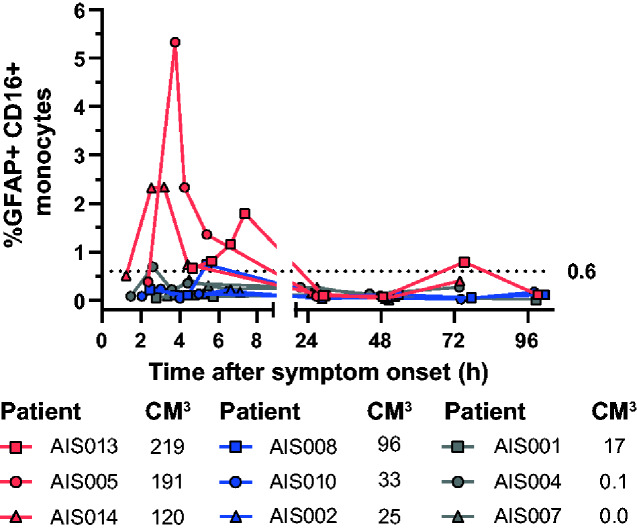
Diagnosis and monitoring of primary brain tumours, brain metastasis and acute ischaemic stroke all require invasive, burdensome and costly diagnostics, frequently lacking adequate sensitivity, particularly during disease monitoring. Monocytes are known to migrate to damaged tissues, where they act as tissue macrophages, continuously scavenging, phagocytizing and digesting apoptotic cells and other tissue debris. We hypothesize that upon completion of their tissue-cleaning task, these tissue macrophages might migrate via the lymph system to the bloodstream, where they can be detected and evaluated for their phagolysosomal contents. We discovered a blood monocyte subpopulation carrying the brain-specific glial fibrillary acidic protein in glioma patients and in patients with brain metastasis and evaluated the diagnostic potential of this finding. Blood samples were collected in a cross-sectional study before or during surgery from adult patients with brain lesions suspected of glioma. Together with blood samples from healthy controls, these samples were flowing cytometrically evaluated for intracellular glial fibrillary acidic protein in monocyte subsets. Acute ischaemic stroke patients were tested at multiple time points after onset to evaluate the presence of glial fibrillary acidic protein-carrying monocytes in other forms of brain tissue damage. Clinical data were collected retrospectively. High-grade gliomas (N = 145), brain metastasis (N = 21) and large stroke patients (>100 cm3) (N = 3 versus 6; multiple time points) had significantly increased frequencies of glial fibrillary acidic protein+CD16+ monocytes compared to healthy controls. Based on both a training and validation set, a cut-off value of 0.6% glial fibrillary acidic protein+CD16+ monocytes was established, with 81% sensitivity (95% CI 75-87%) and 85% specificity (95% CI 80-90%) for brain lesion detection. Acute ischaemic strokes of >100 cm3 reached >0.6% of glial fibrillary acidic protein+CD16+ monocytes within the first 2-8 h after hospitalization and subsided within 48 h. Glioblastoma patients with >20% glial fibrillary acidic protein+CD16+ non-classical monocytes had a significantly shorter median overall survival (8.1 versus 12.1 months). Our results and the available literature, support the hypothesis of a tissue-origin of these glial fibrillary acidic protein-carrying monocytes. Blood monocytes carrying glial fibrillary acidic protein have a high sensitivity and specificity for the detection of brain lesions and for glioblastoma patients with a decreased overall survival. Furthermore, their very rapid response to acute tissue damage identifies large areas of ischaemic tissue damage within 8 h after an ischaemic event. These studies are the first to report the clinical applicability for brain tissue damage detection through a minimally invasive diagnostic method, based on blood monocytes and not serum markers, with direct consequences for disease monitoring in future (therapeutic) studies and clinical decision making in glioma and acute ischaemic stroke patients.
Keywords: acute ischemic stroke; glioma; metastatic CNS tumour; minimal invasive diagnostics; neuroimmunology.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Ahmad O, Wardlaw J, Fau-Whiteley WN, Whiteley WN. Correlation of levels of neuronal and glial markers with radiological measures of infarct volume in ischaemic stroke: a systematic review. Cerebrovasc Dis 2012; 33: 47–54. - PubMed
-
- Almeida J, Bueno C, Alguero MC, Sanchez ML, de Santiago M, Escribano L, et al. Comparative analysis of the morphological, cytochemical, immunophenotypical, and functional characteristics of normal human peripheral blood lineage(-)/CD16(+)/HLA-DR(+)/CD14(-/lo) cells, CD14(+) monocytes, and CD16(-) dendritic cells. Clinical Immunol 2001; 100: 325–38. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous