

Call Center Remote Triage by Nurse Practitioners Was Associated With Fewer Subsequent Face-to-Face Healthcare Visits
- PMID: 33501532
- PMCID: PMC7837076
- DOI: 10.1007/s11606-020-06536-0
Call Center Remote Triage by Nurse Practitioners Was Associated With Fewer Subsequent Face-to-Face Healthcare Visits
Abstract
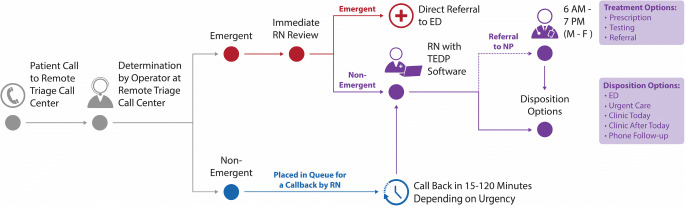
Background: In 2015, the Veterans Health Administration (VHA) incorporated nurse practitioners (NPs) into remote triage call centers to supplement registered nurse (RN)-handled calls.
Objective: To assess 7-day healthcare use following telephone triage by NPs compared to RNs. We hypothesized that NP clinical decision ability may reduce follow-up healthcare.
Design: Retrospective observational comparative effectiveness study of clinical and administrative databases. NP routed calls were matched to RN calls based on chief complaint with propensity score matching and multivariate count data models, adjusting for differences in call severity and patient comorbidity.
Participants: Callers to a VHA regional call center, April 2015 to March 2019.
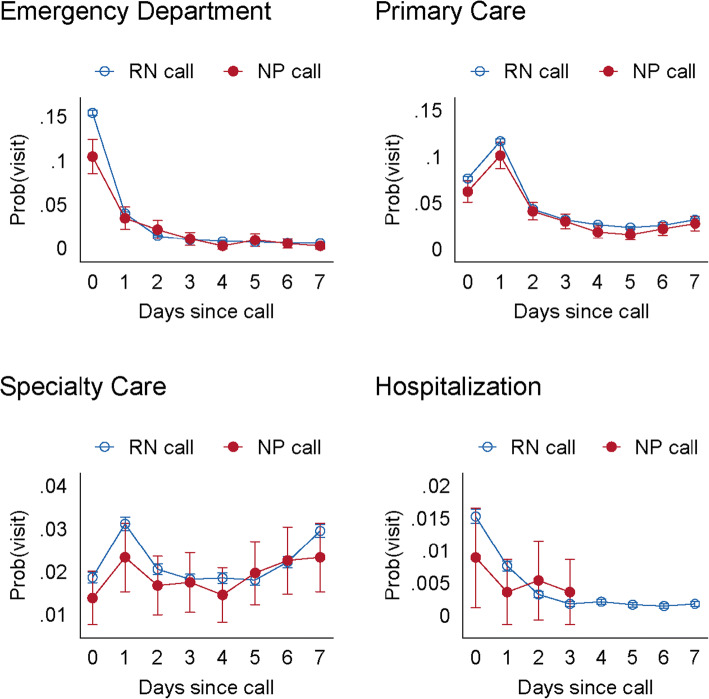
Main measures: Primary care, specialty care, and emergency department (ED) visits plus hospitalizations within 7 days.
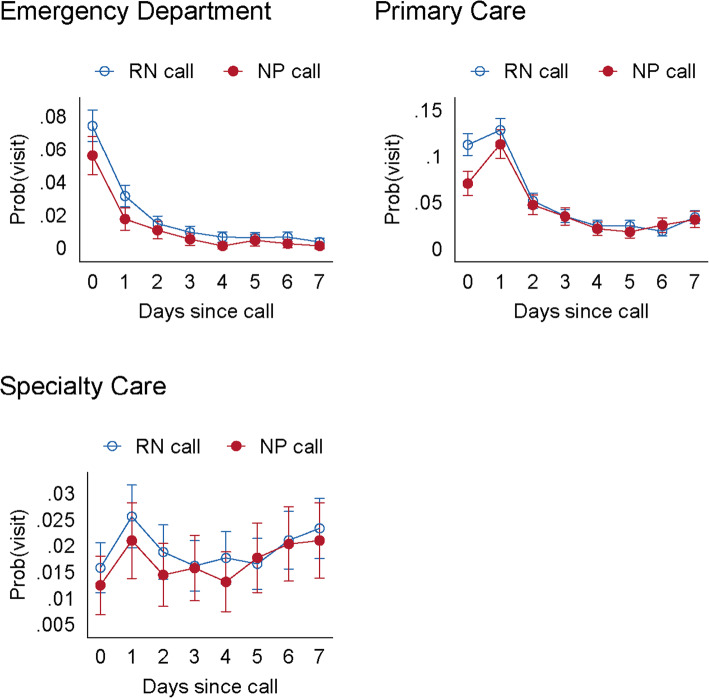
Key results: NP-handled calls (N = 1554) were matched to RN calls (N = 48,024) for the same chief complaint. NP-handled calls, compared to RNs, had lower comorbidities, fewer hospitalizations, and less urgent complaints. Seven-day healthcare use was lower for NP compared to RN calls for specialty care (0.15 vs. 0.20 visits per person [VPP]; p < 0.001), ED (0.11 vs. 0.27 VPP; p < 0.001), and hospitalizations (0.01 vs. 0.04 VPP; p < 0.001), but not primary care (0.43 vs. 0.42 VPP; p = 0.80). In adjusted analyses, estimated avoided in-person visits per 100 calls routed to NPs were 0.7 primary care visits (95% confidence interval [CI] 0.4, 1.0), 2.6 specialty care visits (95% CI 0.0, 5.1), 5.9 ED visits (95% CI 2.7, 9.1), and 1.4 hospital stays (95% CI 0.1, 2.6). Propensity score-matched models comparing NP (N = 1533) to RN (N = 2646) calls had adjusted odds ratios for 7-day healthcare use of 0.75 (primary care), 0.75 (specialty care), and 0.73 (ED) (all p < 0.003).
Conclusion: Incorporating NPs into a call center was associated with lower in-person healthcare use in the subsequent 7 days compared to routine RN-triaged calls.
Keywords: after-hours care; call center; telephone medicine; telephone triage.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Rushton S, Boggan J, Lewinski A, et al. Effectiveness of remote triage: a systematic review. In: Evidence Synthesis Program HSRaDS, Office of Research and Development, Department of Veterans Affairs., ed. Vol VA ESP Project #09-010. Washington, DC2019. - PubMed
-
- Campbell JL, Fletcher E, Britten N, et al. Telephone triage for management of same-day consultation requests in general practice (the ESTEEM trial): a cluster-randomised controlled trial and cost-consequence analysis. Lancet. 2014;384(9957):1859–1868. doi: 10.1016/S0140-6736(14)61058-8. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
