

The Role of Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery
- PMID: 33502455
- PMCID: PMC7841579
- DOI: 10.1001/jamasurg.2020.6363
The Role of Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery
Abstract
Importance: Studies on the prognostic role of hyperthermic intraperitoneal chemotherapy (HIPEC) in pseudomyxoma peritonei (PMP) are currently not available.
Objectives: To evaluate outcomes after cytoreductive surgery (CRS) and HIPEC compared with CRS alone in patients with PMP.
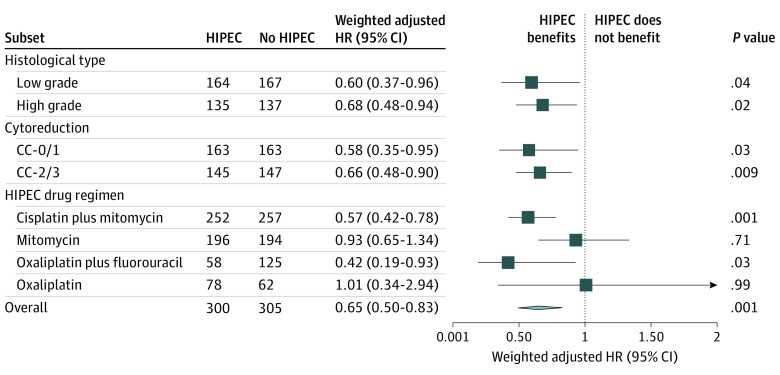
Design, setting, and participants: This cohort study analyzed data from the Peritoneal Surface Oncology Group International (PSOGI) registry, including 1924 patients with histologically confirmed PMP due to an appendiceal mucinous neoplasm. Eligible patients were treated with CRS with or without HIPEC from February 1, 1993, to December 31, 2017, and had complete information on the main prognostic factors and intraperitoneal treatments. Inverse probability treatment weights based on the propensity score for HIPEC treatment containing the main prognostic factors were applied to all models to balance comparisons between the CRS-HIPEC vs CRS-alone groups in the entire series and in the following subsets: optimal cytoreduction, suboptimal cytoreduction, high- and low-grade histologic findings, and different HIPEC drug regimens. Data were analyzed from March 1 to June 1, 2018.
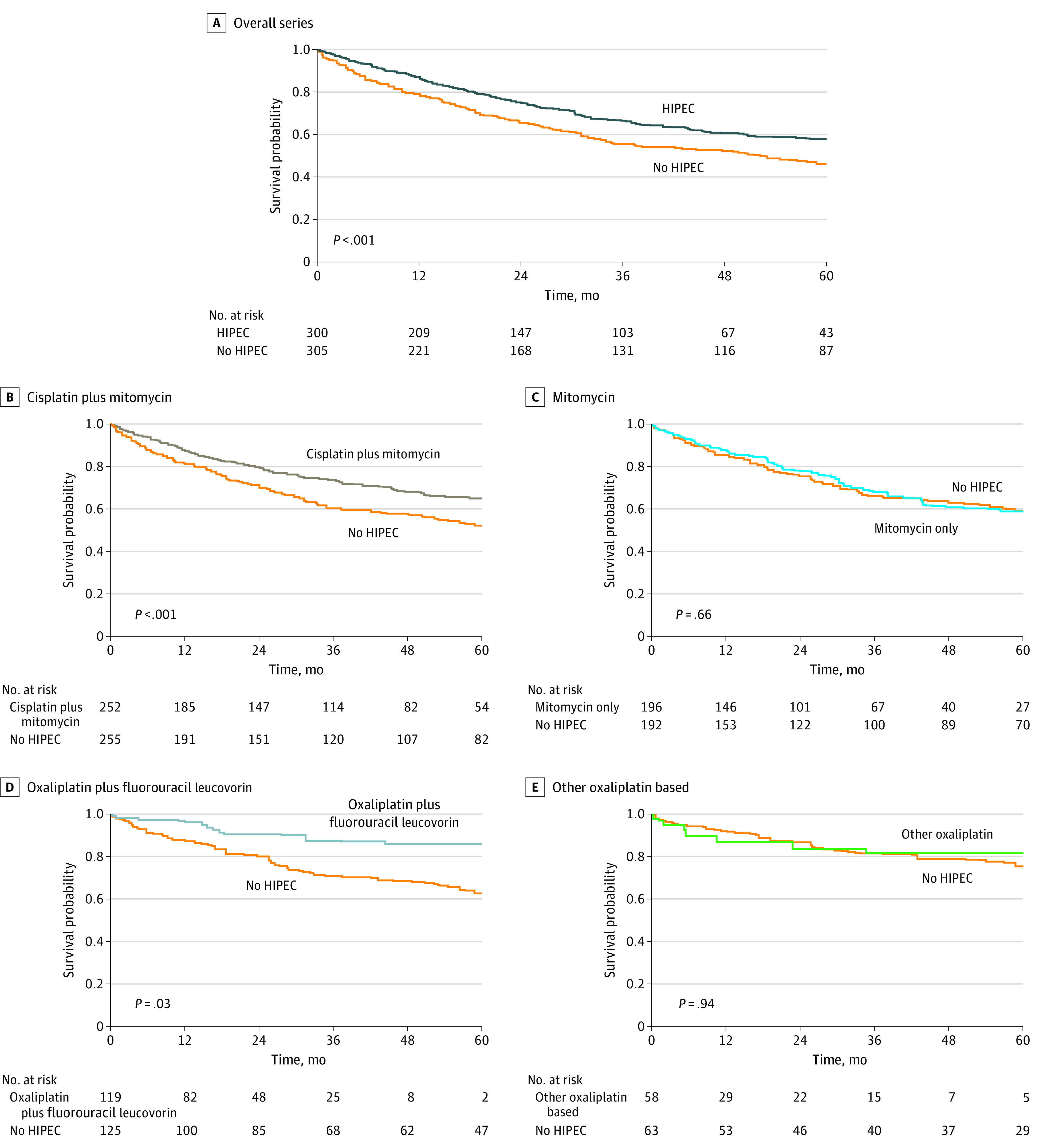
Interventions: HIPEC including oxaliplatin plus combined fluorouracil-leucovorin, cisplatin plus mitomycin, mitomycin, and other oxaliplatin-based regimens.
Main outcomes and measures: Overall survival, severe morbidity (determined using the National Cancer Institute Common Terminology for Adverse Events, version 3.0), return to operating room, and 30- and 90-day mortality. Differences in overall survival were compared using weighted Kaplan-Meier curves, log-rank tests, and Cox proportional hazards multivariable models. A sensitivity analysis was based on the E-value from the results of the main Cox proportional hazards model. Differences in surgical outcomes were compared using weighted multivariable logistic models.
Results: Of the 1924 patients included in the analysis (997 [51.8%] men; median age, 56 [interquartile range extremes (IQRE), 45-65] years), 376 were in the CRS-alone group and 1548 in the CRS-HIPEC group. Patients with CRS alone were older (median age, 60 [IQRE, 48-70] vs 54 [IQRE, 44-63] years), had less lymph node involvement (14 [3.7%] vs 119 [7.7%]), received more preoperative systemic chemotherapy (198 [52.7%] vs 529 [34.2%]), and had higher proportions of high-grade disease (179 [47.6%] vs 492 [31.8%]) and suboptimal cytoreduction residual disease (grade 3, 175 [46.5%] vs 117 [7.6%]). HIPEC was not associated with a higher risk of worse surgical outcomes except with mitomycin, with higher odds of morbidity (1.99; 95% CI, 1.25-3.19; P = .004). HIPEC was associated with a significantly better overall survival in all subsets (adjusted hazard ratios [HRs], 0.60-0.68, with 95% CIs not crossing 1.00). The weighted 5-year overall survival was 57.8% (95% CI, 50.8%-65.7%) vs 46.2% (95% CI, 40.3%-52.8%) for CRS-HIPEC and CRS alone, respectively (weighted HR, 0.65; 95% CI, 0.50-0.83; P < .001; E-value, 2.03). Such prognostic advantage was associated with oxaliplatin plus fluorouracil-leucovorin (HR, 0.42; 95% CI, 0.19-0.93; P = .03) and cisplatin plus mitomycin (HR, 0.57; 95% CI, 0.42-0.78; P = .001) schedules.
Conclusions and relevance: In this cohort study, HIPEC was associated with better overall survival when performed after CRS in PMP, generally without adverse effects on surgical outcomes.
Conflict of interest statement
Figures

Comment in
-
Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery.JAMA Surg. 2021 Mar 1;156(3):e206364. doi: 10.1001/jamasurg.2020.6364. Epub 2021 Mar 10. JAMA Surg. 2021. PMID: 33502464 No abstract available.
References
-
- Carr NJ, McCarthy WF, Sobin LH. Epithelial noncarcinoid tumors and tumor-like lesions of the appendix: a clinicopathologic study of 184 patients with a multivariate analysis of prognostic factors. Cancer. 1995;75:757-768. doi: 10.1002/1097-0142(19950201)75:3<757::AID-CNCR2820750303>3.0.CO;2-F - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
