

Long-Term Health-Related Quality of Life (HRQoL) After Redo-Fundoplication
- PMID: 33502565
- PMCID: PMC8026436
- DOI: 10.1007/s00268-021-05954-3
Long-Term Health-Related Quality of Life (HRQoL) After Redo-Fundoplication
Erratum in
-
Correction to: Long-Term Health-Related Quality of Life (HRQoL) After Redo-Fundoplication.World J Surg. 2021 May;45(5):1503. doi: 10.1007/s00268-021-06009-3. World J Surg. 2021. PMID: 33620542 Free PMC article. No abstract available.
Abstract
Background: We aim to shed light on long-term subjective outcomes after re-operations for failed fundoplication.
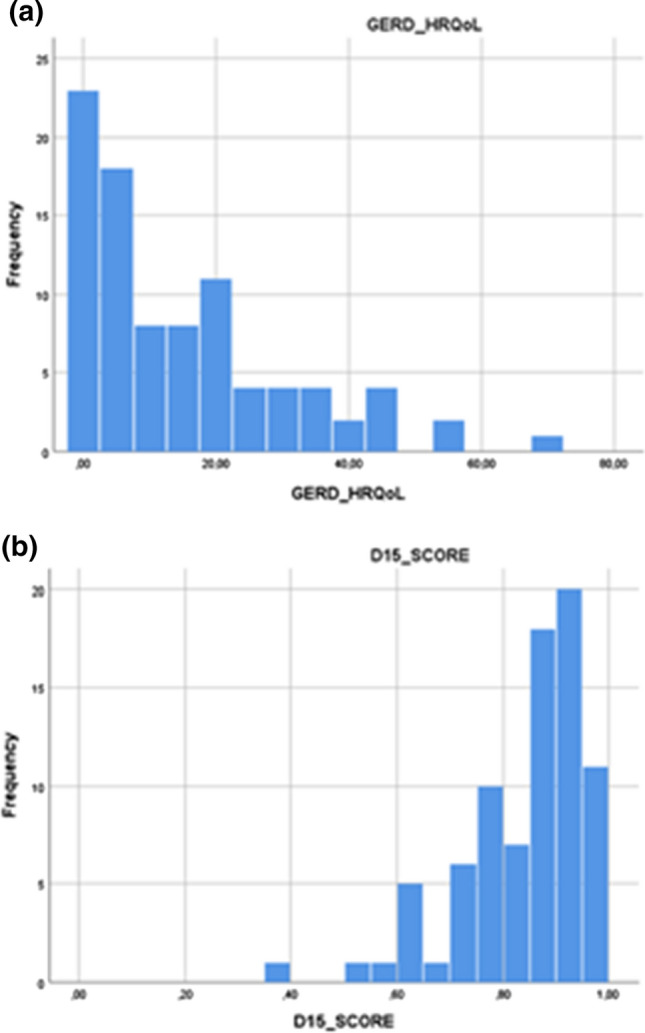
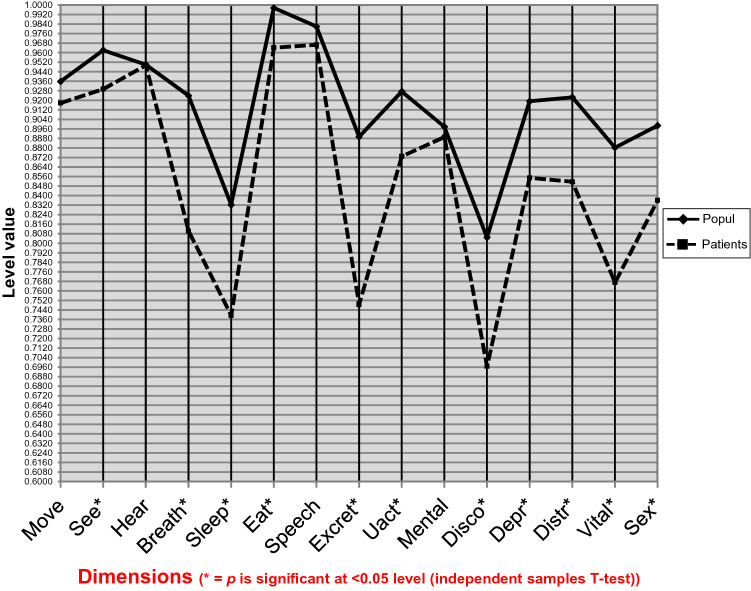
Methods: 1809 patients were operated on for hiatal hernia and/or gastroesophageal reflux disease (GERD) at the Helsinki University Hospital between 2000 and 2017. 111 (6%) of these had undergone a re-operation for a failed antireflux operation. Overall, HRQoL was assessed in 89 patients at the latest follow-up using the generic 15D© instrument. The results were compared to a sample of the general population, weighted to reflect the age and gender distribution of patients. Disease-specific HRQoL was assessed using the GERD-HRQoL questionnaire. We studied variation in the overall HRQoL with respect to disease-specific HRQoL and known patients' parameters using univariate and multivariable linear regression models.
Results: The median postoperative follow-up period was 9.3 years. All patients were operated on laparoscopically (6% conversion rate), and 87% were satisfied with the re-operation. Postoperative complications were minimal (5%). Twelve patients (11%) underwent a second re-operation. The median GERD-HRQoL score was nine. In multivariable analysis, four variables were independently associated with the 15D score, suggesting a decrease in the 15D score with increasing GERD-HRQoL score, increasing Charlson Comorbidity Index (CCI) and the presence of chronic pain syndrome (CPS) and depression.
Conclusion: Re-do LF is a safe procedure in experienced hands and may offer acceptable long-term alleviation in patients with recurring symptoms after antireflux surgery. Decreased HRQoL in the long run is related to recurring GERD and co-morbidities.
Conflict of interest statement
Harri Sintonen is the developer of the 15D and obtains royalties from its electronic versions. Tom Scheinin is a member of the Nordic Colorectal Advisory Board (Johnson & Johnson). The other authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Quality of life and gastric acid-suppression medication post-laparoscopic fundoplication: a ten years retrospective study.Acta Chir Belg. 2022 Oct;122(5):321-327. doi: 10.1080/00015458.2020.1860551. Epub 2022 Jul 20. Acta Chir Belg. 2022. PMID: 33534655
-
[Surgery of the hiatal hernia and gastroesophageal reflux dinase, Nissen or Toupet?].Rozhl Chir. 2015 Dec;94(12):510-5. Rozhl Chir. 2015. PMID: 26767901 Czech.
-
REDO LAPAROSCOPIC ANTIREFLUX SURGERY IN PATIENTS WITH HIATAL HERNIA.Georgian Med News. 2021 Mar;(312):23-26. Georgian Med News. 2021. PMID: 33964820
-
[Reccurent reflux … and other problems following fundoplication: indication for re-operation].Zentralbl Chir. 2014 Feb;139(1):43-9. doi: 10.1055/s-0031-1283982. Epub 2012 May 21. Zentralbl Chir. 2014. PMID: 22614229 Review. German.
-
The evolution and long-term results of laparoscopic antireflux surgery for the treatment of gastroesophageal reflux disease.JSLS. 2010 Jul-Sep;14(3):332-41. doi: 10.4293/108680810X12924466007007. JSLS. 2010. PMID: 21333184 Free PMC article. Review.
Cited by
-
The impact of obesity on gastroesophageal reflux disease recurrence following re-operative anti-reflux surgery.Surg Endosc. 2024 Nov;38(11):6389-6395. doi: 10.1007/s00464-024-11182-2. Epub 2024 Aug 30. Surg Endosc. 2024. PMID: 39214878
-
Does crural repair with biosynthetic mesh improve outcomes of revisional surgery for recurrent hiatal hernia?Hernia. 2024 Oct;28(5):1687-1695. doi: 10.1007/s10029-024-03023-x. Epub 2024 Mar 29. Hernia. 2024. PMID: 38551795 Free PMC article.
-
Laparoscopic Surgery for Recurrent Hiatal Hernia: Clinical Outcomes and Quality of Life.J Gastrointest Surg. 2022 Apr;26(4):917-920. doi: 10.1007/s11605-021-05165-0. Epub 2021 Oct 19. J Gastrointest Surg. 2022. PMID: 34668163 No abstract available.
-
Malpractice claims after antireflux surgery and paraesophageal hernia repair: a population-based analysis.Surg Endosc. 2024 Feb;38(2):624-632. doi: 10.1007/s00464-023-10572-2. Epub 2023 Nov 27. Surg Endosc. 2024. PMID: 38012443 Free PMC article.
-
Potentially inappropriate medication use and comorbidity in association with quality of life in community-dwelling older people: a cross-sectional study in Iran.BMC Prim Care. 2025 May 20;26(1):175. doi: 10.1186/s12875-025-02882-2. BMC Prim Care. 2025. PMID: 40394468 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
