

Underfilling decreases left ventricular function in pulmonary arterial hypertension
- PMID: 33502652
- PMCID: PMC8105202
- DOI: 10.1007/s10554-020-02143-6
Underfilling decreases left ventricular function in pulmonary arterial hypertension
Abstract
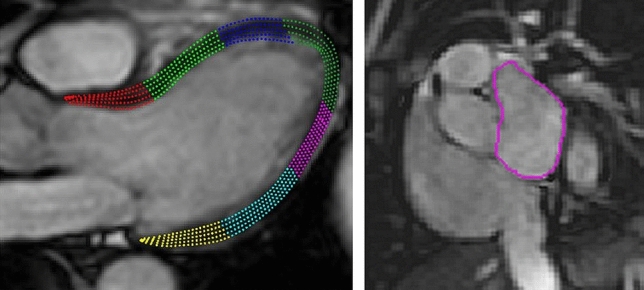
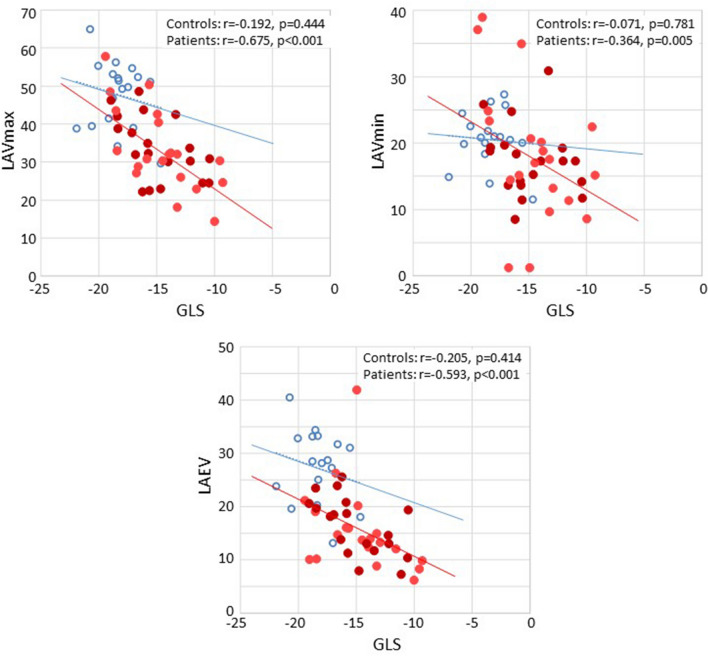
To evaluate the association between impaired left ventricular (LV) longitudinal function and LV underfilling in patients with pulmonary arterial hypertension (PAH). Thirty-nine patients with PAH and 18 age and sex-matched healthy controls were included. LV volume and left atrial volume (LAV) were delineated in short-axis cardiac magnetic resonance (CMR) cine images. LV longitudinal function was assessed from atrio-ventricular plane displacement (AVPD) and global longitudinal strain (GLS) was assessed using feature tracking in three long-axis views. LV filling was assessed by LAV and by pulmonary artery wedge pressure (PAWP) using right heart catheterisation. Patients had a smaller LAV, LV volume and stroke volume as well as a lower LV-AVPD and LV-GLS than controls. PAWP was 6 [IQR 5--9] mmHg in patients. LV ejection fraction did not differ between groups. LV stroke volume correlated with LV-AVPD (r = 0.445, p = .001), LV-GLS (r = - 0.549, p < 0.0001) and LAVmax (r = .585, p < 0.0001). Furthermore, LV-AVPD (r = .598) and LV-GLS (r = - 0.675) correlated with LAVmax (p < 0.0001 for both). Neither LV-AVPD, LV-GLS, LAVmax nor stroke volume correlated with PAWP. Impaired LV longitudinal function was associated with low stroke volume, low PAWP and a small LAV in PAH. Small stroke volumes and LAV, together with normal LA pressure, implies that the mechanism causing reduced LV longitudinal function is underfilling rather than an intrinsic LV dysfunction in PAH.
Keywords: Cardiac magnetic resonance imaging; Feature tracking strain; Left atrial volume; Left ventricular dysfunction; Pulmonary hypertension.
Conflict of interest statement
None of the authors have any conflict of interest related to this manuscript.
Figures


Similar articles
-
Left ventricular dysfunction in pulmonary arterial hypertension is attributed to underfilling rather than intrinsic myocardial disease: a CMR 2D phase contrast study.Sci Rep. 2024 Jul 27;14(1):17280. doi: 10.1038/s41598-024-68254-5. Sci Rep. 2024. PMID: 39068288 Free PMC article.
-
Decreased biventricular longitudinal strain in patients with systemic sclerosis is mainly caused by pulmonary hypertension and not by systemic sclerosis per se.Clin Physiol Funct Imaging. 2019 May;39(3):215-225. doi: 10.1111/cpf.12561. Epub 2019 Jan 16. Clin Physiol Funct Imaging. 2019. PMID: 30597705 Free PMC article.
-
Atrioventricular plane displacement and regional function to predict outcome in pulmonary arterial hypertension.Int J Cardiovasc Imaging. 2022 Oct;38(10):2235-2248. doi: 10.1007/s10554-022-02616-w. Epub 2022 Apr 23. Int J Cardiovasc Imaging. 2022. PMID: 37726454 Free PMC article.
-
Quantitative assessment of systolic left ventricular function with speckle-tracking echocardiography in adult patients with repaired aortic coarctation.Int J Cardiovasc Imaging. 2016 May;32(5):777-87. doi: 10.1007/s10554-016-0838-8. Epub 2016 Jan 16. Int J Cardiovasc Imaging. 2016. PMID: 26780661 Free PMC article.
-
Left ventricular underfilling in PAH: A potential indicator for adaptive-to-maladaptive transition.Pulm Circ. 2023 Nov 30;13(4):e12309. doi: 10.1002/pul2.12309. eCollection 2023 Oct. Pulm Circ. 2023. PMID: 38045097 Free PMC article. Review.
Cited by
-
The sine transform is the sine qua non of the pulmonary and systemic pressure relationship.Front Cardiovasc Med. 2023 May 26;10:1120330. doi: 10.3389/fcvm.2023.1120330. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37304951 Free PMC article.
-
Exercise and hypoxia unmask pulmonary vascular disease and right ventricular dysfunction in a 10- to 12-week-old swine model of neonatal oxidative injury.J Physiol. 2022 Sep;600(17):3931-3950. doi: 10.1113/JP282906. Epub 2022 Aug 11. J Physiol. 2022. PMID: 35862359 Free PMC article.
-
Increased biventricular hemodynamic forces in precapillary pulmonary hypertension.Sci Rep. 2022 Nov 19;12(1):19933. doi: 10.1038/s41598-022-24267-6. Sci Rep. 2022. PMID: 36402861 Free PMC article.
-
Ventricular Function and Cardio-Ankle Vascular Index in Patients With Pulmonary Artery Hypertension.Vasc Health Risk Manag. 2022 Dec 28;18:889-904. doi: 10.2147/VHRM.S385536. eCollection 2022. Vasc Health Risk Manag. 2022. PMID: 36597509 Free PMC article.
-
Non-invasive imaging techniques for early diagnosis of bilateral cardiac dysfunction in pulmonary hypertension: current crests, future peaks.Front Cardiovasc Med. 2024 May 9;11:1393580. doi: 10.3389/fcvm.2024.1393580. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38784167 Free PMC article. Review.
References
-
- Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, Aboyans V, Vaz Carneiro A, Achenbach S, Agewall S, Allanore Y, Asteggiano R, Paolo Badano L, Albert Barberà J, Bouvaist H, Bueno H, Byrne RA, Carerj S, Castro G, Erol Ç, Falk V, Funck-Brentano C, Gorenflo M, Granton J, Iung B, Kiely DG, Kirchhof P, Kjellstrom B, Landmesser U, Lekakis J, Lionis C, Lip GY, Orfanos SE, Park MH, Piepoli MF, Ponikowski P, Revel MP, Rigau D, Rosenkranz S, Völler H, Luis Zamorano J. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
-
- Rådegran G, Kjellström B, Ekmehag B, Larsen F, Rundqvist B, Blomquist SB, Gustafsson C, Hesselstrand R, Karlsson M, Kornhall B, Nisell M, Persson L, Ryftenius H, Selin M, Ullman B, Wall K, Wikström G, Willehadson M, Jansson K, Stefan Söderberg on behalf of SveFPH and SPAHR (2016) Characteristics and survival of adult Swedish PAH and CTEPH patients 2000–2014. Scand Cardiovasc J 50:243–250 - PubMed
-
- Kylhammar D, Kjellström B, Hjalmarsson C, Söderberg S, Wikström G, Nisell M, Jansson K, Rådegran G, on behalf of SveFPH and SPAHR (2018) A comprehensive risk stratification at early follow-up determines prognosis in pulmonary arterial hypertension. Eur Heart J 39:4175–4181 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
