

Prophylactic anticoagulants for people hospitalised with COVID-19
- PMID: 33502773
- PMCID: PMC8166900
- DOI: 10.1002/14651858.CD013739
Prophylactic anticoagulants for people hospitalised with COVID-19
Update in
-
Anticoagulants for people hospitalised with COVID-19.Cochrane Database Syst Rev. 2022 Mar 4;3(3):CD013739. doi: 10.1002/14651858.CD013739.pub2. Cochrane Database Syst Rev. 2022. PMID: 35244208 Free PMC article.
Abstract
Background: Coronavirus disease 2019 (COVID-19) is a serious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The primary manifestation is respiratory insufficiency that can also be related to diffuse pulmonary microthrombosis in people with COVID-19. This disease also causes thromboembolic events, such as pulmonary embolism, deep venous thrombosis, arterial thrombosis, catheter thrombosis, and disseminated intravascular coagulopathy. Recent studies have indicated a worse prognosis for people with COVID-19 who developed thromboembolism. Anticoagulants are medications used in the prevention and treatment of venous or arterial thromboembolic events. Several drugs are used in the prophylaxis and treatment of thromboembolic events, such as heparinoids (heparins or pentasaccharides), vitamin K antagonists and direct anticoagulants. Besides their anticoagulant properties, heparinoids have an additional anti-inflammatory potential, that may affect the clinical evolution of people with COVID-19. Some practical guidelines address the use of anticoagulants for thromboprophylaxis in people with COVID-19, however, the benefit of anticoagulants for people with COVID-19 is still under debate.
Objectives: To assess the effects of prophylactic anticoagulants versus active comparator, placebo or no intervention, on mortality and the need for respiratory support in people hospitalised with COVID-19.
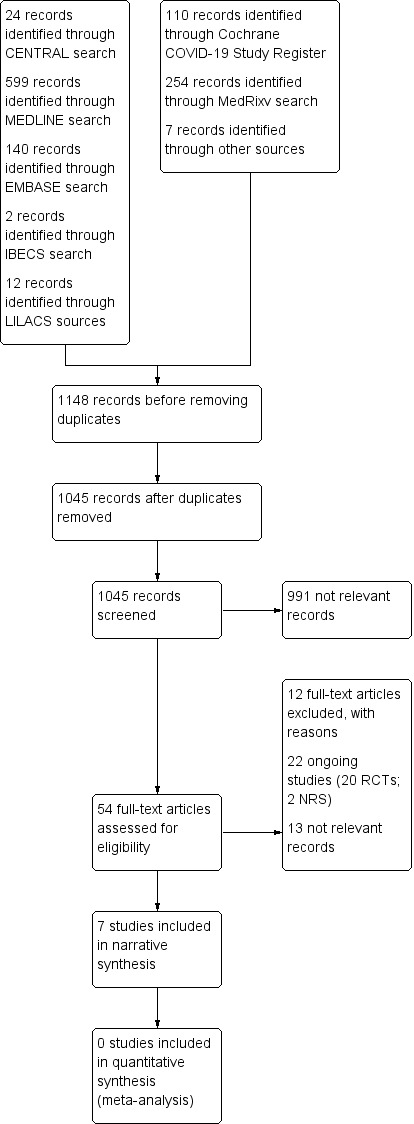
Search methods: We searched CENTRAL, MEDLINE, Embase, LILACS and IBECS databases, the Cochrane COVID-19 Study Register and medRxiv preprint database from their inception to 20 June 2020. We also checked reference lists of any relevant systematic reviews identified and contacted specialists in the field for additional references to trials.
Selection criteria: Randomised controlled trials (RCTs), quasi-RCTs, cluster-RCTs and cohort studies that compared prophylactic anticoagulants (heparin, vitamin K antagonists, direct anticoagulants, and pentasaccharides) versus active comparator, placebo or no intervention for the management of people hospitalised with COVID-19. We excluded studies without a comparator group. Primary outcomes were all-cause mortality and need for additional respiratory support. Secondary outcomes were mortality related to COVID-19, deep vein thrombosis (DVT), pulmonary embolism, major bleeding, adverse events, length of hospital stay and quality of life.
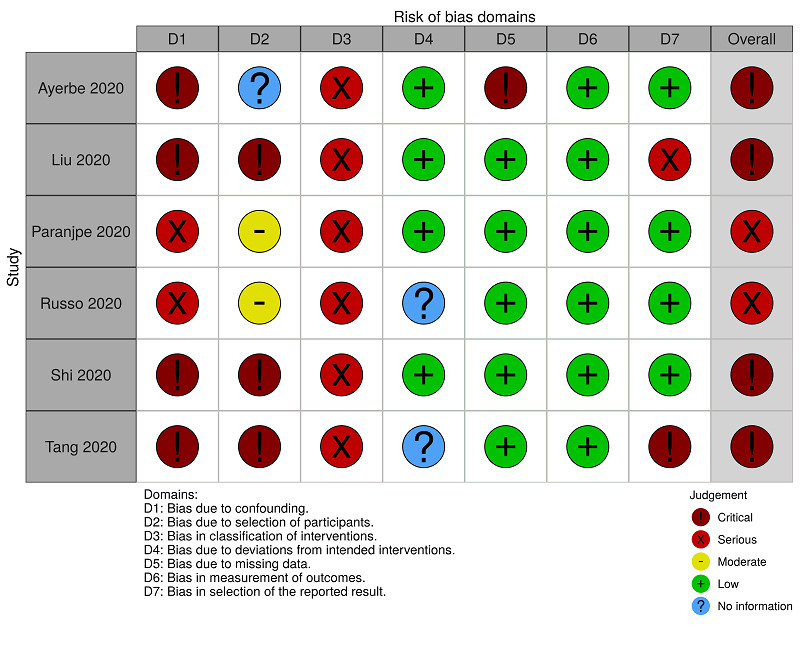
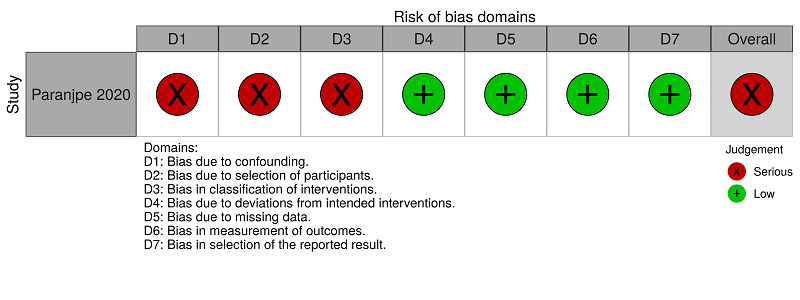
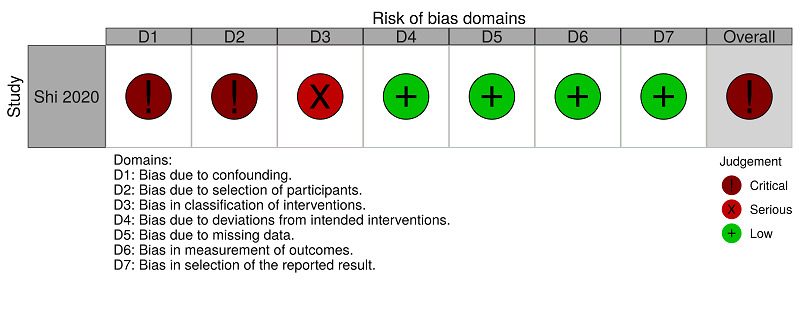
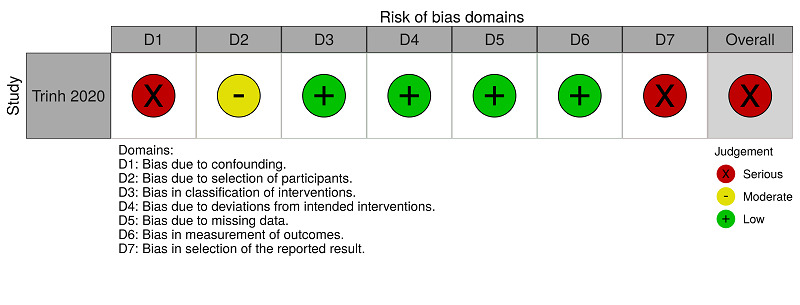
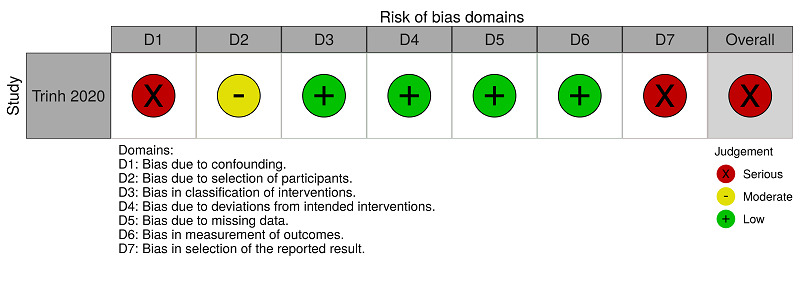
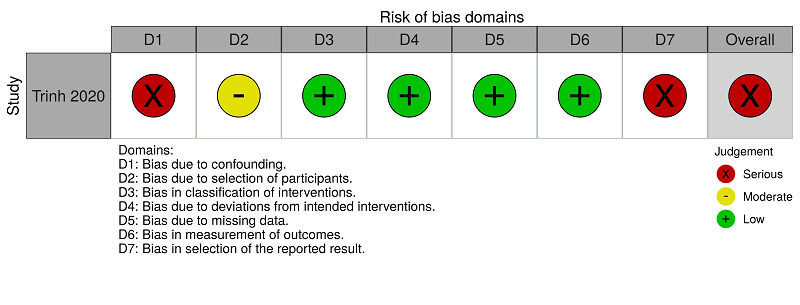
Data collection and analysis: We used standard Cochrane methodological procedures. We used ROBINS-I to assess risk of bias for non-randomised studies (NRS) and GRADE to assess the certainty of evidence. We reported results narratively.
Main results: We identified no RCTs or quasi-RCTs that met the inclusion criteria. We included seven retrospective NRS (5929 participants), three of which were available as preprints. Studies were conducted in China, Italy, Spain and the USA. All of the studies included people hospitalised with COVID-19, in either intensive care units, hospital wards or emergency departments. The mean age of participants (reported in 6 studies) ranged from 59 to 72 years. Only three included studies reported the follow-up period, which varied from 8 to 35 days. The studies did not report on most of our outcomes of interest: need for additional respiratory support, mortality related to COVID-19, DVT, pulmonary embolism, adverse events, and quality of life. Anticoagulants (all types) versus no treatment (6 retrospective NRS, 5685 participants) One study reported a reduction in all-cause mortality (adjusted odds ratio (OR) 0.42, 95% confidence interval (CI) 0.26 to 0.66; 2075 participants). One study reported a reduction in mortality only in a subgroup of 395 people who required mechanical ventilation (hazard ratio (HR) 0.86, 95% CI 0.82 to 0.89). Three studies reported no differences in mortality (adjusted OR 1.64, 95% CI 0.92 to 2.92; 449 participants; unadjusted OR 1.66, 95% CI 0.76 to 3.64; 154 participants and adjusted risk ratio (RR) 1.15, 95% CI 0.29 to 2.57; 192 participants). One study reported zero events in both intervention groups (42 participants). The overall risk of bias for all-cause mortality was critical and the certainty of the evidence was very low. One NRS reported bleeding events in 3% of the intervention group and 1.9% of the control group (OR 1.62, 95% CI 0.96 to 2.71; 2773 participants; low-certainty evidence). Therapeutic-dose anticoagulants versus prophylactic-dose anticoagulants (1 retrospective NRS, 244 participants) The study reported a reduction in all-cause mortality (adjusted HR 0.21, 95% CI 0.10 to 0.46) and a lower absolute rate of death in the therapeutic group (34.2% versus 53%). The overall risk of bias for all-cause mortality was serious and the certainty of the evidence was low. The study also reported bleeding events in 31.7% of the intervention group and 20.5% of the control group (OR 1.8, 95% CI 0.96 to 3.37; low-certainty evidence). Ongoing studies We found 22 ongoing studies in hospital settings (20 RCTs, 14,730 participants; 2 NRS, 997 participants) in 10 different countries (Australia (1), Brazil (1), Canada (2), China (3), France (2), Germany (1), Italy (4), Switzerland (1), UK (1) and USA (6)). Twelve ongoing studies plan to report mortality and six plan to report additional respiratory support. Thirteen studies are expected to be completed in December 2020 (6959 participants), eight in July 2021 (8512 participants), and one in December 2021 (256 participants). Four of the studies plan to include 1000 participants or more.
Authors' conclusions: There is currently insufficient evidence to determine the risks and benefits of prophylactic anticoagulants for people hospitalised with COVID-19. Since there are 22 ongoing studies that plan to evaluate more than 15,000 participants in this setting, we will add more robust evidence to this review in future updates.
INTRODUÇÃO: A doença coronavírus 2019 (COVID‐19) é uma doença grave causada por pelo coronavírus 2 da síndrome respiratória aguda grave (SARS‐CoV‐2). Sua manifestação primária é a insuficiência respiratória, que também pode estar relacionada à microtrombose pulmonar difusa vista em pacientes com COVID‐19. A doença também causa eventos tromboembólicos, tais como embolia pulmonar, trombose venosa profunda, trombose arterial, trombose de cateter e coagulopatia intravascular disseminada. Estudos recentes indicam que os pacientes com COVID‐19 que desenvolvem tromboembolismo têm um pior prognóstico. Os anticoagulantes são medicamentos utilizados na prevenção e no tratamento de eventos tromboembólicos venosos ou arteriais. Vários medicamentos são utilizados na profilaxia e no tratamento de eventos tromboembólicos, tais como heparinoides (heparinas ou pentasacarídeos), antagonistas da vitamina K e anticoagulantes diretos. Além de suas propriedades anticoagulantes, os heparinoides têm um potencial anti‐inflamatório adicional. Essa propriedade poderia afetar a evolução clínica dos pacientes com COVID‐19. Algumas diretrizes clínicas abordam o uso de anticoagulantes para tromboprofilaxia em pacientes com COVID‐19. Porém, o benefício dos anticoagulantes para esses pacientes ainda está em debate. OBJETIVOS: Avaliar os efeitos do uso de anticoagulantes profiláticos versus um comparador ativo, placebo ou nenhuma intervenção, na mortalidade e na necessidade de suporte respiratório em pacientes internados com COVID‐19. MÉTODOS DE BUSCA: Fizemos buscas nas seguintes bases de dados eletrônicas desde seu início até 20 de junho de 2020: CENTRAL, MEDLINE, Embase, LILACS e IBECS, Cochrane COVID‐19 Study Register e a base de dados de pré‐impressão medRxiv. Também revisamos as listas de referências das revisões sistemáticas relevantes e contatamos especialistas da área em busca de referências adicionais de ensaios clínicos. CRITÉRIO DE SELEÇÃO: Incluímos ensaios clínicos randomizados controlados (ECRs), quasi‐randomizados, ECR tipo cluster e coortes. Os estudos deveriam comparar o uso de anticoagulantes profiláticos (heparina, antagonistas da vitamina K, anticoagulantes diretos e pentasacarídeos) versus um comparador ativo, placebo ou nenhuma intervenção, em pacientes hospitalizadas com COVID‐19. Excluímos estudos sem um grupo de comparação. Os desfechos primários foram mortalidade por todas as causas e a necessidade de suporte respiratório adicional. Os desfechos secundários foram mortalidade relacionada à COVID‐19, trombose venosa profunda (TVP), embolia pulmonar, sangramento importante, eventos adversos, tempo de internação hospitalar e qualidade de vida. COLETA DOS DADOS E ANÁLISES: Adotamos os procedimentos metodológicos padrão da Cochrane. Utilizamos o ROBINS‐I para avaliar o risco de viés dos estudos não randomizados (NRS) e o GRADE para avaliar a certeza da evidência. Apresentamos os resultados de forma narrativa. PRINCIPAIS RESULTADOS: Não identificamos nenhum ECR ou quasi‐randomizado que preenchessem os critérios de inclusão. Incluímos sete estudos retrospectivos não randomizados (5929 participantes). Três desses estudos estavam disponíveis como pré‐impressões. Os estudos foram conduzidos na China, Itália, Espanha e nos EUA. Todos os estudos incluíram pessoas hospitalizadas com COVID‐19, em unidades de terapia intensiva, enfermarias ou departamentos de emergência. A idade média dos participantes (relatada em 6 estudos) variou de 59 a 72 anos. Apenas três estudos relataram qual foi o período de acompanhamento, que variou de 8 a 35 dias. Os estudos não relataram a maioria dos nossos desfechos de interesse: necessidade de suporte respiratório adicional, mortalidade relacionada à COVID‐19, TVP, embolia pulmonar, eventos adversos e qualidade de vida. Anticoagulantes (todos os tipos) versus nenhum tratamento (6 estudos não randomizados retrospectivos, 5685 participantes) Um estudo relatou redução na mortalidade por todas as causas (odds ratio ajustado (OR) 0,42, intervalo de confiança (IC) 95% 0,26 a 0,66; 2075 participantes). Um estudo relatou redução na mortalidade apenas num subgrupo de 395 pessoas que necessitaram de ventilação mecânica (hazard ratio (HR) 0,86, IC 95% 0,82 a 0,89). Três estudos não encontraram diferenças na mortalidade (OR ajustado 1,64, IC 95% 0,92 a 2,92; 449 participantes; OR não ajustado 1,66, IC 95% 0,76 a 3,64; 154 participantes e razão de risco ajustada (RR) 1,15, IC 95% 0,29 a 2,57; 192 participantes). Um estudo não teve nenhum caso de morte nos dois grupos (42 participantes). O risco geral de viés para mortalidade por todas as causas é crítico e a qualidade (certeza) da evidência é muito baixa. Um estudo não randomizado relatou que 3% dos participantes do grupo intervenção e 1,9% daqueles do grupo controle tiveram eventos de sangramento (OR 1,62, IC 95% 0,96 a 2,71; 2773 participantes; evidência de baixa qualidade). Anticoagulantes em dose terapêutica versus anticoagulantes em dose profilática (1 estudo retrospectivo não randomizado, 244 participantes) O estudo relatou redução na mortalidade por todas as causas (HR ajustado 0,21, IC 95% 0,10 a 0,46) e menor taxa absoluta de morte no grupo tratado com dose terapêutica (34,2% versus 53%). O risco geral de viés para mortalidade por todas as causas é grave e a qualidade da evidência é baixa. O estudo também relatou eventos de sangramento em 31,7% dos participantes do grupo intervenção e em 20,5% daqueles no grupo controle (OR 1,8, IC 95% 0,96 a 3,37; evidência de baixa qualidade). Estudos em andamento Encontramos 22 estudos em andamento em ambientes hospitalares (20 ECRs, 14.730 participantes; 2 estudos não randomizados, 997 participantes). Esses estudos estão sendo realizados em 10 países diferentes: Austrália (1), Brasil (1), Canadá (2), China (3), França (2), Alemanha (1), Itália (4), Suíça (1), Reino Unido (1) e EUA (6). Doze estudos em andamento pretendem avaliar mortalidade e seis vão avaliar suporte respiratório adicional. Espera‐se que 13 estudos sejam concluídos em dezembro de 2020 (6959 participantes), oito em julho de 2021 (8512 participantes) e um em dezembro de 2021 (256 participantes). Quatro dos estudos planejam incluir 1000 participantes ou mais. CONCLUSÃO DOS AUTORES: Atualmente não há evidência suficiente sobre os riscos e benefícios do uso de anticoagulantes profiláticos para pacientes hospitalizados com COVID‐19. Como há 22 estudos em andamento que planejam avaliar mais de 15.000 participantes internados, a evidência das futuras atualizações desta revisão será mais robusta.
บทนำ: โรคโคโรนาไวรัส 2019 (COVID‐19) เป็นโรคร้ายแรงที่เกิดจากกลุ่มอาการทางเดินหายใจเฉียบพลันรุนแรง coronavirus 2 (SARS‐CoV‐2) อาการหลักคือ ระบบทางเดินหายใจทำงานไม่เพียงพอ ซึ่งอาจเกี่ยวข้องกับการเกิด microthrombosis ในปอดแบบกระจายในผู้ที่เป็น COVID‐19 โรคนี้ยังทำให้เกิดภาวะลิ่มเลือดอุดตัน เช่นเส้นเลือดในปอดอุดตัน หลอดเลือดดำส่วนลึกอุดตัน เส้นเลือดแดงอุดตัน สายสวนอุดตัน และการแข็งตัวของหลอดเลือดผิดปกติทั่วร่างกาย การศึกษาเมื่อเร็ว ๆ นี้ชี้ให้เห็นการพยากรณ์โรคที่แย่ลงสำหรับผู้ที่ติดเชื้อ COVID‐19 ซึ่งเป็นโรคลิ่มเลือดอุดตัน ยาต้านการแข็งตัวของเลือดเป็นยาที่ใช้ในการป้องกันและรักษาภาวะลิ่มเลือดอุดตันในหลอดเลือดดำหรือหลอดเลือดแดง มีการใช้ยาหลายชนิดในการป้องกันและการรักษาภาวะลิ่มเลือดอุดตันเช่น heparinoids (heparins หรือ pentasaccharides) ยาต้านวิตามินเค และยาต้านการแข็งตัวของเลือดโดยตรง นอกจากคุณสมบัติในการต้านการแข็งตัวของเลือดแล้ว heparinoids ยังมีฤทธิ์ต้านการอักเสบเพิ่มเติม ซึ่งอาจส่งผลต่อการเปลี่ยนแปลงทางคลินิกของผู้ที่เป็น COVID‐19 แนวทางปฏิบัติบางส่วน กล่าวถึงการใช้ยาต้านการแข็งตัวของเลือดในผู้ที่เป็นโรค COVID‐19 อย่างไรก็ตามประโยชน์ของยาต้านการแข็งตัวของเลือดสำหรับผู้ที่ติดเชื้อ COVID‐19 ยังคงเป็นที่ถกเถียงกันอยู่ วัตถุประสงค์: เพื่อประเมินผลของยาต้านการแข็งตัวของเลือด เมื่อเทียบกับตัวเปรียบเทียบที่ออกฤทธิ์ ยาหลอกหรือไม่มีการรักษา ต่อการเสียชีวิตและความจำเป็นในการช่วยหายใจในผู้ที่เข้ารับการรักษาในโรงพยาบาลด้วย COVID‐19 วิธีการสืบค้น: เราสืบค้นฐานข้อมูล CENTRAL, MEDLINE, Embase, LILACS และ IBECS, Cochrane COVID‐19 Study Register และฐานข้อมูล medRxiv preprint ตั้งแต่เริ่มต้นจนถึง 20 มิถุนายน 2020 นอกจากนี้เรายังตรวจสอบรายการอ้างอิงของการทบทวนวรรณกรรมอย่างเป็นระบบที่เกี่ยวข้องที่พบ และติดต่อผู้เชี่ยวชาญในสาขานั้นสำหรับเอกสารอ้างอิงเพิ่มเติมเกี่ยวกับการทดลอง เกณฑ์การคัดเลือก: การทดลองแบบสุ่มที่มีกลุ่มควบคุม (RCTs), quasi‐RCTs, cluster‐RCTs และการศึกษาแบบ cohort ที่เปรียบเทียบยาต้านการแข็งตัวของเลือด (heparin, vitamin K antagonists, direct anticoagulants และ pentasaccharides) เทียบกับ active comparator, placebo หรือไม่มีการรักษาใด ๆ สำหรับการดูแลผู้ที่เข้ารับการรักษาในโรงพยาบาลด้วย COVID ‐19 เราไม่รวมการศึกษาที่ไม่มีกลุ่มเปรียบเทียบ ผลลัพธ์หลักคือการเสียชีวิตจากทุกสาเหตุ และความจำเป็นต้องได้รับการช่วยหายใจเพิ่มเติม ผลลัพธ์รอง ได้แก่ การเสียชีวิตจาก COVID‐19, ลิ่มเลือดอุดตันในหลอดเลือดดำ (DVT), เส้นเลือดอุดตันในปอด, เลือดออกที่สำคัญ, เหตุการณ์ไม่พึงประสงค์, ระยะเวลาในการนอนโรงพยาบาลและคุณภาพชีวิต การรวบรวมและวิเคราะห์ข้อมูล: เราใช้ระเบียบวิธีการวิจัยตามมาตรฐานของ Cochrane เราใช้ ROBINS‐I เพื่อประเมินความเสี่ยงของอคติสำหรับการศึกษาแบบไม่สุ่ม (NRS) และ GRADE เพื่อประเมินความเชื่อมั่นของหลักฐาน เรารายงานผลแบบบรรยาย ผลการวิจัย: เราไม่พบ RCT หรือ quasi RCT ที่ตรงตามเกณฑ์การคัดเลือก เรารวม retrospective NRS 7 รายการ (ผู้เข้าร่วม 5929 คน) ซึ่ง 3 รายการ อยู่ในรูปแบบของฉบับร่างหรือเป็นฉบับก่อนที่ตีพิมพ์ การศึกษาดำเนินการในจีน อิตาลี สเปน และสหรัฐอเมริกา การศึกษาทั้งหมดรวมผู้ที่เข้ารับการรักษาในโรงพยาบาลด้วย COVID‐19 ทั้งในหอผู้ป่วยหนัก หอผู้ป่วยในโรงพยาบาลหรือแผนกฉุกเฉิน อายุเฉลี่ยของผู้เข้าร่วมการศึกษา (รายงานใน 6 การศึกษา) อยู่ระหว่าง 59 ถึง 72 ปี มีการศึกษาเพียง 3 รายการเท่านั้นที่รายงานระยะเวลาติดตามผลซึ่งแตกต่างกันไปตั้งแต่ 8 ถึง 35 วัน การศึกษาไม่ได้รายงานเกี่ยวกับผลลัพธ์ที่น่าสนใจส่วนใหญ่ของเรา: ความต้องการการช่วยหายใจเพิ่มเติม การเสียชีวิตที่เกี่ยวข้องกับ COVID‐19, DVT, เส้นเลือดอุดตันในปอด, เหตุการณ์ไม่พึงประสงค์และคุณภาพชีวิต ยาต้านการแข็งตัวของเลือด (ทุกประเภท) เทียบกับไม่มีการรักษา (Retrospective NRS 6 รายการ ผู้เข้าร่วม 5685 คน) การศึกษา 1 รายการรายงานว่าการเสียชีวิตจากทุกสาเหตุลดลง (อัตราส่วนที่ปรับแล้ว (OR) 0.42, ช่วงความเชื่อมั่น 95% (CI) 0.26 ถึง 0.66; ผู้เข้าร่วม 2075 คน) การศึกษา 1 รายการรายงานว่าการลดลงของอัตราการตายเฉพาะในกลุ่มย่อย 395 คนที่ต้องใช้เครื่องช่วยหายใจ (harzard ratio (HR) 0.86, 95% CI 0.82 ถึง 0.89) การศึกษา 3 รายการรายงานว่าไม่มีความแตกต่างในการตาย (adjusted OR 1.64, 95% CI 0.92 ถึง 2.92; ผู้เข้าร่วม 449 คน; unadjusted OR 1.66, 95% CI 0.76 ถึง 3.64; ผู้เข้าร่วม 154 คนและ adjusted risk ratio (RR) 1.15, 95% CI 0.29 ถึง 2.57; ผู้เข้าร่วม 192 คน) การศึกษา 1 รายการรายงานว่าไม่มีเหตุการณ์ในทั้งสองกลุ่มการรักษา (ผู้เข้าร่วม 42 คน) ความเสี่ยงของการมีอคติโดยรวมสำหรับการเสียชีวิตจากทุกสาเหตสูงมาก และความเชื่อมั่นของหลักฐานต่ำมาก NRS 1 รายการรายงานุการเลือดออกใน 3% ของกลุ่มรักษา และ 1.9% ของกลุ่มควบคุม (OR 1.62, 95% CI 0.96 ถึง 2.71; ผู้เข้าร่วม 2773 คน; หลักฐานที่มีความเชื่อมั่นต่ำ) ยาต้านการแข็งตัวของเลือดในขนาดที่ใช้รักษาเทียบกับยาต้านการแข็งตัวของเลือดในขนาดที่ใช้ป้องกันโรค (1 retrospective NRS ผู้เข้าร่วม 244 คน) การศึกษารายงานการลดลงของการเสียชีวิตจากทุกสาเหตุ (adjusted HR 0.21, 95% CI 0.10 ถึง 0.46) และอัตราการเสียชีวิตลดลงในกลุ่มรักษา (34.2% เทียบกับ 53%) ความเสี่ยงโดยรวมของอคติสำหรับการเสียชีวิตจากทุกสาเหตสูงมาก และความเชื่อมั่นของหลักฐานต่ำ การศึกษาได้รายงานการมีเลือดออกใน 31.7% ของกลุ่มรักษา และ 20.5% ของกลุ่มควบคุม (OR 1.8, 95% CI 0.96 ถึง 3.37; หลักฐานที่มีความเชื่อมั่นต่ำ) การศึกษาที่กำลังดำเนินการ เราพบการศึกษาที่กำลังดำเนินการ 22 เรื่องในสถานพยาบาล (20 RCTs ผู้เข้าร่วม 14,730 คน; 2 NRS ผู้เข้าร่วม 997 คน) ใน 10 ประเทศ (ออสเตรเลีย (1), บราซิล (1), แคนาดา (2), จีน (3), ฝรั่งเศส (2) , เยอรมนี (1), อิตาลี (4), สวิตเซอร์แลนด์ (1), สหราชอาณาจักร (1) และสหรัฐอเมริกา (6)) การศึกษาที่กำลังดำเนินการ 12 รายการวางแผนที่จะรายงานการเสียชีวิต และ 6 รายการวางแผนที่จะรายงานการสนับสนุนทางเดินหายใจเพิ่มเติม การศึกษา 13 รายการคาดว่าจะแล้วเสร็จในเดือนธันวาคม 2020 (ผู้เข้าร่วม 6959 คน) 8 การศึกษาในเดือนกรกฎาคม 2021 (ผู้เข้าร่วม 8512 คน) และหนึ่งในเดือนธันวาคม 2021 (ผู้เข้าร่วม 256 คน) การศึกษา 4 รายการมีแผนจะรวมผู้เข้าร่วม 1000 คนขึ้นไป ข้อสรุปของผู้วิจัย: ขณะนี้ยังไม่มีหลักฐานเพียงพอที่จะประเมินุความเสี่ยงและประโยชน์ของยาต้านการแข็งตัวของเลือดสำหรับผู้ที่เข้ารับการรักษาในโรงพยาบาลด้วย COVID‐19 เนื่องจากมีการศึกษาที่กำลังดำเนินการ 22 รายการที่วางแผนจะประเมินผู้เข้าร่วมมากกว่า 15,000 คนในบริบทนี้ เราจะเพิ่มหลักฐานที่ชัดเจนยิ่งขึ้นในการตรวจสอบนี้ในการอัปเดตในอนาคต.
پیشینه: بیماری کروناویروس 2019 (COVID‐19) یک بیماری جدی است که توسط سندرم حاد تنفسی شدید کروناویروس ‐2 (SARS‐CoV‐2) ایجاد میشود. تظاهرات اولیه آن نارسایی تنفسی است که میتواند با میکروترومبوز منتشر ریوی در افراد مبتلا به COVID‐19 نیز مرتبط باشد. این بیماری همچنین باعث وقوع حوادث ترومبوآمبولیک، مانند آمبولی ریوی، ترومبوز وریدی عمقی، ترومبوز شریانی، ترومبوز کاتتر، و انعقاد داخل عروقی منتشر میشود. مطالعات اخیر پیشآگهی بدتری را برای افراد مبتلا به COVID‐19 که به ترومبوآمبولی دچار شدهاند، نشان دادهاند. آنتیکوآگولانتها، داروهایی هستند که در پیشگیری و درمان حوادث ترومبوآمبولی وریدی یا شریانی استفاده میشوند. داروهای متعددی در پروفیلاکسی و درمان حوادث ترومبوآمبولیک استفاده میشوند، مانند هپارینوئیدها (هپارینها یا پنتاساکاریدها (pentasaccharides))، آنتاگونیستهای ویتامین K و آنتیکوآگولانتهای مستقیم. هپارینوئیدها، علاوه بر خاصیت آنتیکوآگولانتی خود، پتانسیل ضد‐التهابی بیشتری هم دارند، که ممکن است بر تکامل بالینی افراد مبتلا به COVID‐19 تأثیر بگذارد. برخی از دستورالعملهای عملی استفاده از آنتیکوآگولانتها را برای ترومبوپروفیلاکسی در افراد مبتلا به COVID‐19 توصیه میکنند، با این حال، مزیت آنتیکوآگولانتها برای افراد مبتلا به COVID‐19 هنوز مورد بحث است. اهداف: ارزیابی اثرات آنتیکوآگولانتهای پروفیلاکتیک در مقایسه با مقایسه کننده فعال، دارونما (placebo) یا عدم مداخله، بر مورتالیتی و نیاز به حمایت تنفسی در بیماران بستری با COVID‐19. روشهای جستوجو: ما بانکهای اطلاعاتی CENTRAL؛ MEDLINE؛ Embase؛ LILACS و IBECS، پایگاه ثبت مطالعات COVID‐19 در کاکرین، و بانک اطلاعاتی پیش از چاپ medRxiv را از بدو تاسیس آنها تا 20 جون 2020 جستوجو کردیم. همچنین فهرست منابع مرورهای سیستماتیک مرتبط را که شناسایی شدند، بررسی کرده و برای یافتن منابع بیشتر، با متخصصان این زمینه تماس گرفتیم. معیارهای انتخاب: کارآزماییهای تصادفیسازی و کنترل شده (randomised controlled trials; RCTs)، شبه‐RCTها، RCTهای خوشهای و مطالعات کوهورت که آنتیکوآگولانتهای پروفیلاکتیک (هپارین، آنتاگونیستویتامین K، آنتیکوآگولانتهای مستقیم و پنتاساکاریدها) را در برابر مقایسه کننده فعال، دارونما یا عدم مداخله برای مدیریت افراد بستری با COVID‐19 مقایسه کردند. ما مطالعات بدون گروه مقایسه کننده را حذف کردیم. پیامدهای اولیه عبارت بودند از مورتالیتی به هر علتی و نیاز به حمایت تنفسی بیشتر. پیامدهای ثانویه، مورتالیتی مرتبط با COVID‐19، ترومبوز ورید عمقی (DVT)، آمبولی ریوی، خونریزی عمده، عوارض جانبی، طول مدت بستری در بیمارستان و کیفیت زندگی بودند. گردآوری و تجزیهوتحلیل دادهها: از پروسیجرهای استاندارد روششناسی کاکرین استفاده شد. ما از ROBINS‐I برای ارزیابی خطر سوگیری (bias) در مطالعات غیر‐تصادفیسازی شده (NRS) و روش درجهبندی توصیه، ارزیابی، توسعه و ارزشیابی (GRADE) برای ارزیابی قطعیت شواهد استفاده کردیم. نتایج را به صورت روایتگونه گزارش کردیم. نتایج اصلی: ما هیچ RCT یا شبه‐RCTای را شناسایی نکردیم که معیارهای ورود را داشته باشند. ما هفت NRS گذشتهنگر (5929 شرکتکننده) را وارد کردیم، که سه مورد از آنها به صورت پیش از چاپ (preprint) در دسترس بودند. مطالعات در چین، ایتالیا، اسپانیا و ایالات متحده انجام شدند. همه مطالعات شامل افرادی بودند که با COVID‐19، در بخشهای مراقبت ویژه، بخشهای بیمارستان یا بخشهای اورژانس، بستری بودند. میانگین سنی شرکتکنندگان (در 6 مطالعه گزارش شد) از 59 تا 72 سال متغیر بود. فقط سه مطالعه وارد شده، دوره پیگیری را گزارش کردند، که از 8 تا 35 روز متفاوت بود. این مطالعات اغلب پیامدهای مورد نظر ما را گزارش نکردند: نیاز به حمایت تنفسی بیشتر، مورتالیتی مرتبط با COVID‐19؛ DVT، آمبولی ریوی، عوارض جانبی، و کیفیت زندگی. آنتیکوآگولانتها (همه انواع) در مقابل عدم درمان (شش NRS گذشتهنگر، 5685 شرکتکننده) یک مطالعه کاهش را در مورتالیتی به هر علتی گزارش کرد (نسبت شانس تعدیل شده (OR): 0.42؛ 95% فاصله اطمینان (CI): 0.26 تا 0.66؛ 2075 شرکتکننده). یک مطالعه کاهش مورتالیتی را فقط در زیرگروهی با 395 نفر که به تهویه مکانیکی نیاز داشتند، گزارش کرد (نسبت خطر (HR): 0.86؛ 95% CI؛ 0.82 تا 0.89). سه مطالعه هیچ تفاوتی را در میزان مورتالیتی گزارش نکردند (OR تعدیل شده: 1.64؛ 95% CI؛ 0.92 تا 2.92؛ 449 شرکتکننده؛ OR تعدیل نشده: 1.66؛ 95% CI؛ 0.76 تا 3.64؛ 154 شرکتکننده و نسبت خطر (RR) تعدیل شده: 1.15؛ 95% CI؛ 0.29 تا 2.57؛ 192 شرکتکننده). یک مطالعه وقوع صفر مورد حوادث را در هر دو گروه مداخله (42 شرکتکننده) گزارش کرد. خطر کلی سوگیری برای مورتالیتی به هر علتی، بحرانی و قطعیت شواهد بسیار پائین بود. یک NRS، حوادث خونریزی دهنده را در 3% از شرکتکنندگان گروه مداخله و 1.9% از افراد گروه کنترل گزارش کرد (OR: 1.62؛ 95% CI؛ 0.96 تا 2.71؛ 2773 شرکتکننده؛ شواهد با قطعیت پائین). آنتیکوآگولانتها با دوز درمانی در مقابل آنتیکوآگولانتها با دوز پروفیلاکتیک (یک NRS گذشتهنگر، 244 شرکتکننده) این مطالعه کاهش را در مورتالیتی به هر علتی (HR تعدیل شده: 0.21؛ 95% CI؛ 0.10 تا 0.46) و میزان مطلق پائینتر مرگ را در گروه دوز درمانی (34.2% در مقابل 53%) نشان داد. خطر کلی سوگیری برای مورتالیتی به هر علتی، جدی و قطعیت شواهد پائین بود. یک NRS همچنین حوادث خونریزی دهنده را در 31.7% از افراد گروه مداخله و 20.5% از بیماران گروه کنترل گزارش کرد (OR: 1.8؛ 95% CI؛ 0.96 تا 3.37؛ شواهد با قطعیت پائین). مطالعات در حال انجام ما 22 مطالعه در حال انجام را در شرایط بیمارستانی (20 RCT؛ 14,730 شرکتکننده؛ 2 NRS؛ 997 شرکتکننده) در 10 کشور مختلف (استرالیا (1)، برزیل (1)، کانادا (2)، چین (3)، فرانسه (2)، آلمان (1)، ایتالیا (4)، سوئیس (1)، انگلیس (1)، و ایالات متحده آمریکا (6)) یافتیم. دوازده مطالعه در حال انجام قصد دارند مورتالیتی و شش مطالعه میخواهند نیاز به پشتیبانی تنفسی بیشتر را گزارش کنند. انتظار میرود سیزده مطالعه در دسامبر 2020 (6959 شرکتکننده)، هشت مورد در جولای 2021 (8512 شرکتکننده)، و یک مطالعه در دسامبر 2021 (256 شرکتکننده) به پایان برسند. چهار مورد از این مطالعات شامل 1000 شرکتکننده یا بیشتر هستند. نتیجهگیریهای نویسندگان: در حال حاضر شواهد کافی برای تعیین خطرات و مزایای آنتیکوآگولانتهای پروفیلاکتیک برای افراد بستری با COVID‐19 وجود ندارد. از آنجا که 22 مطالعه در حال انجام هستند که قصد دارند بیش از 15,000 شرکتکننده را در این شرایط ارزیابی کنند، در بهروزرسانیهای آینده شواهد محکمتری را به این مرور اضافه خواهیم کرد.
Contexte: La maladie à coronavirus 2019 (COVID‐19) est une maladie grave causée par le coronavirus 2 du syndrome respiratoire aigu sévère (SARS‐CoV‐2). La principale manifestation est l'insuffisance respiratoire qui peut également être liée à la microthrombose pulmonaire diffuse chez les personnes atteintes de la COVID‐19. Cette maladie provoque également des événements thromboemboliques, tels que l'embolie pulmonaire, la thrombose veineuse profonde, la thrombose artérielle, la thrombose par cathéter et la coagulopathie intravasculaire disséminée. Des études récentes ont indiqué un pronostic plus défavorable pour les personnes atteintes de la COVID‐19 qui ont développé une thromboembolie. Les anticoagulants sont des médicaments utilisés dans la prévention et le traitement des événements thromboemboliques veineux ou artériels. Plusieurs médicaments sont utilisés dans la prophylaxie et le traitement des événements thromboemboliques, tels que les héparinoïdes (héparines ou pentasaccharides), les antagonistes de la vitamine K et les anticoagulants directs. Outre leurs propriétés anticoagulantes, les héparinoïdes ont un potentiel anti‐inflammatoire supplémentaire, qui pourrait affecter l'évolution clinique des personnes atteintes de COVID‐19. Certaines recommandations de bonnes pratiques cliniques traitent de l'utilisation des anticoagulants pour la thromboprophylaxie chez les personnes atteintes de la COVID‐19, cependant, le bénéfice de l’utilisation des anticoagulants chez les personnes atteintes de la COVID‐19 est toujours en débat.
Objectifs: Évaluer les effets des anticoagulants à dose prophylactique par rapport à un comparateur actif, au placebo ou à l’absence d’intervention, sur la mortalité et le besoin d'assistance respiratoire chez les personnes hospitalisées pour la COVID‐19. STRATÉGIE DE RECHERCHE DOCUMENTAIRE: Nous avons effectué des recherches dans les bases de données CENTRAL, MEDLINE, Embase, LILACS et IBECS, dans le registre d'étude Cochrane sur la COVID‐19 et dans la base de données de prépublications medRxiv depuis leur création jusqu'au 20 juin 2020. Nous avons également vérifié les références bibliographiques de toutes les revues systématiques pertinentes identifiées et avons contacté les spécialistes du domaine pour obtenir des références supplémentaires sur les essais. CRITÈRES DE SÉLECTION: Essais contrôlés randomisés (ECR), essais quasi‐randomisés, essais randomisés en grappes et études de cohortes qui comparent les anticoagulants à dose prophylactique (héparine, antagonistes de la vitamine K, anticoagulants directs et pentasaccharides) à un comparateur actif, un placebo ou à l’absence d’intervention dans la prise en charge des personnes hospitalisées pour la COVID‐19. Nous avons exclu les études sans groupe de comparaison. Les critères de jugement principaux sont la mortalité toutes causes confondues et la nécessité d'une assistance respiratoire supplémentaire. Les critères de jugement secondaires étaient la mortalité liée à la COVID‐19, la thrombose veineuse profonde (TVP), l'embolie pulmonaire, les hémorragies graves, les événements indésirables, la durée du séjour à l'hôpital et la qualité de vie. RECUEIL ET ANALYSE DES DONNÉES: Nous avons utilisé les procédures méthodologiques standards de Cochrane. Nous avons utilisé ROBINS‐I pour évaluer le risque de biais pour les études non randomisées et GRADE pour évaluer le niveau de confiance des données probantes. Nous avons rapporté les résultats de manière narrative. RÉSULTATS PRINCIPAUX: Nous n'avons pas identifié d’ECR ou d’essais quasi‐randomisés répondant aux critères d'inclusion. Nous avons inclus sept études non randomisées rétrospectives (5 929 participants), dont trois étaient disponibles sous forme de prépublication. Les études ont été menées en Chine, en Italie, en Espagne et aux États‐Unis. Toutes les études ont porté sur des personnes hospitalisées pour la COVID‐19, dans des unités de soins intensifs, des services hospitaliers ou des services d'urgence. L'âge moyen des participants (indiqué dans 6 études) se situait entre 59 et 72 ans. Seules trois études incluses ont rapporté la période de suivi, qui variait de 8 à 35 jours. Les études n'ont pas rapporté la plupart de nos critères de jugement d'intérêt: besoin d'une assistance respiratoire supplémentaire, mortalité liée à la COVID‐19, TVP, embolie pulmonaire, événements indésirables et qualité de vie. Anticoagulants (tous types) par rapport à l’absence de traitement (6 études non randomisées rétrospectives, 5 685 participants) Une étude a rapporté une réduction de la mortalité toutes causes confondues (rapport des cotes ajusté (RC) 0,42, intervalle de confiance (IC) à 95% 0,26 à 0,66 ; 2 075 participants). Une étude a rapporté une réduction de la mortalité uniquement dans un sous‐groupe de 395 personnes qui avaient besoin d'une ventilation mécanique (rapport des risques instantanés (HR) 0,86, IC à 95% 0,82 à 0,89). Trois études n'ont pas rapporté de différence sur la mortalité (RC ajusté de 1,64, IC à 95 % de 0,92 à 2,92 ; 449 participants ; RC non ajusté de 1,66, IC à 95 % de 0,76 à 3,64 ; 154 participants et risque relatif (RR) ajusté de 1,15, IC à 95 % de 0,29 à 2,57 ; 192 participants). Une étude n’a pas rapporté d’événement dans les deux groupes d'intervention (42 participants). Le risque global de biais pour la mortalité toutes causes confondues était critique et le niveau de confiance des données probantes était très faible. Une étude non randomisée a rapporté des événements hémorragiques chez 3 % du groupe d'intervention et 1,9 % du groupe témoin (RC 1,62, IC à 95 % 0,96 à 2,71 ; 2 773 participants ; données probantes d’un niveau de confiance faible). Anticoagulants à dose thérapeutique par rapport aux anticoagulants à dose prophylactique (1 étude non randomisée rétrospective, 244 participants) L'étude a rapporté une réduction de la mortalité toutes causes confondues (HR ajusté 0,21, IC à 95 % 0,10 à 0,46) et un taux absolu de décès plus faible dans le groupe thérapeutique (34,2 % contre 53 %). Le risque global de biais pour la mortalité toutes causes confondues était sérieux et le niveau de confiance des données probantes était faible. L'étude a également rapporté des événements hémorragiques chez 31,7 % du groupe d’intervention et 20,5 % du groupe témoin (RC 1,8, IC à 95 % 0,96 à 3,37 ; données probantes d’un niveau de confiance faible). Etudes en cours Nous avons trouvé 22 études en cours en milieu hospitalier (20 ECR, 14 730 participants ; 2 études non randomisées, 997 participants) dans 10 pays différents (Australie (1), Brésil (1), Canada (2), Chine (3), France (2), Allemagne (1), Italie (4), Suisse (1), Royaume‐Uni (1) et États‐Unis (6)). Douze études en cours prévoient de rapporter la mortalité et six prévoient de rapporter l'assistance respiratoire supplémentaire. Treize études devraient être achevées en décembre 2020 (6 959 participants), huit en juillet 2021 (8 512 participants) et une en décembre 2021 (256 participants). Quatre de ces études prévoient d'inclure 1 000 participants ou plus.
Conclusions des auteurs: Il n'y a actuellement pas suffisamment de données probantes pour déterminer les risques et les bénéfices des anticoagulants à dose prophylactique chez les personnes hospitalisées pour la COVID‐19. Étant donné que 22 études qui sont en cours prévoient d'évaluer plus de 15 000 participants dans ce contexte, nous ajouterons des données probantes plus robustes à cette revue dans de futures mises à jour.
Antecedentes: La enfermedad por coronavirus 2019 (covid‐19) es grave y está causada por el síndrome respiratorio agudo grave por coronavirus 2 (SARS‐CoV‐2, del inglés). La manifestación principal es la insuficiencia respiratoria, que también se puede relacionar con la microtrombosis pulmonar difusa en personas con covid‐19. Esta enfermedad también causa eventos tromboembólicos como embolia pulmonar, trombosis venosa profunda, trombosis arterial, trombosis del catéter y coagulopatía intravascular diseminada. Estudios recientes han indicado un peor pronóstico para las personas con covid‐19 que desarrollaron tromboembolia. Los anticoagulantes son fármacos utilizados para la prevención y el tratamiento de eventos tromboembólicos venosos o arteriales. En la profilaxis y el tratamiento de los eventos tromboembólicos se utilizan varios medicamentos como los heparinoides (heparinas o pentasacáridos), los antagonistas de la vitamina K y los anticoagulantes directos. Además de sus propiedades anticoagulantes, los heparinoides tienen un potencial antiinflamatorio adicional, que puede afectar la evolución clínica de las personas con covid‐19. Algunas guías de práctica clínica abordan el uso de anticoagulantes para la tromboprofilaxis en personas con covid‐19; sin embargo, el efecto beneficioso de los anticoagulantes para las personas con covid‐19 aún es objeto de debate.
Objetivos: Evaluar los efectos de los anticoagulantes profilácticos versus un comparador activo, placebo o ninguna intervención, sobre la mortalidad y la necesidad de asistencia respiratoria en personas hospitalizadas con covid‐19. MÉTODOS DE BÚSQUEDA: Se hicieron búsquedas en las bases de datos CENTRAL, MEDLINE, Embase, LILACS e IBECS, el Registro Cochrane de estudios de covid‐19 (Cochrane COVID‐19 Study Register) y en la bases de datos de prepublicaciones medRxiv, desde su creación hasta el 20 de junio de 2020. También se verificaron las listas de referencias de cualquier revisión sistemática relevante identificada y se estableció contacto con expertos en el tema para obtener referencias adicionales de ensayos. CRITERIOS DE SELECCIÓN: Ensayos controlados aleatorizados (ECA), cuasiECA, ECA grupales y estudios de cohortes que compararon anticoagulantes profilácticos (heparina, antagonistas de la vitamina K, anticoagulantes directos y pentasacáridos) versus comparador activo, placebo o ninguna intervención para el tratamiento de personas hospitalizadas con covid‐19. Se excluyeron los estudios sin un grupo de comparación. Los desenlaces principales fueron la mortalidad por todas las causas y la necesidad de asistencia respiratoria adicional. Los desenlaces secundarios fueron la mortalidad relacionada con covid‐19, la trombosis venosa profunda (TVP) la embolia pulmonar, la hemorragia grave, los eventos adversos, la duración de la estancia hospitalaria y la calidad de vida. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Se utilizaron los procedimientos metodológicos Cochrane estándar. Se utilizó ROBINS‐I para evaluar el riesgo de sesgo para estudios no aleatorizados (ENA) y GRADE para evaluar la certeza de la evidencia. Los resultados se presentaron de forma narrativa.
Resultados principales: No se identificaron ECA ni cuasiECA que cumplieran con los criterios de inclusión. Se incluyeron siete ENA retrospectivos (5929 participantes), tres de las cuales estaban disponibles como prepublicaciones. Los estudios se realizaron en China, EE.UU., España e Italia. Todos los estudios incluyeron personas hospitalizadas con covid‐19 en unidades de cuidados intensivos, salas de hospital o servicios de urgencias. La media de edad de los participantes (informada en seis estudios) varió de 59 a 72 años. Solo tres estudios informaron sobre el período de seguimiento, que varió de ocho a 35 días. Los estudios no informaron la mayoría de los desenlaces de interés: necesidad de asistencia respiratoria, mortalidad relacionada con covid‐19, TVP, embolia pulmonar, episodios adversos y calidad de vida. Anticoagulantes (todos los tipos) versus ningún tratamiento (seis ENA retrospectivos, 5685 participantes) Un estudio informó de una reducción de la mortalidad por todas las causas (odds ratio [OR] 0,42; intervalo de confianza [IC] del 95%: 0,26 a 0,66; 2075 participantes). Un estudio informó de una reducción de la mortalidad solo en un subgrupo de 395 personas que necesitaron ventilación mecánica (cociente de riesgos instantáneos [CRI] 0,86; IC del 95%: 0,82 a 0,89). Tres estudios no informaron diferencias en la mortalidad (OR ajustado 1,64; IC del 95%: 0,92 a 2,92; 449 participantes; OR no ajustado 1,66; IC del 95%: 0,76 a 3,64; 154 participantes, y riesgo relativo [RR] ajustado 1,15; IC del 95%: 0,29 a 2,57; 192 participantes). Un estudio informó cero episodios en ambos grupos de intervención (42 participantes). El riesgo general de mortalidad por todas las causas fue crítico y la certeza de la evidencia fue muy baja. Un ENA informó de episodios de hemorragia en el 3% del grupo de intervención y el 1,9% del grupo control (OR 1,62; IC del 95%: 0,96 a 2,71; 2773 participantes; evidencia de certeza baja). Anticoagulantes en dosis terapéutica versus anticoagulantes en dosis profiláctica (un ENA retrospectivo, 244 participantes) Un estudio informó de una reducción de la mortalidad por todas las causas (CRI ajustado 0,21; IC del 95%: 0,10 a 0,46) y una tasa de mortalidad absoluta menor en el grupo terapéutico (34,2% versus 53%). El riesgo general de mortalidad por todas las causas fue grave y la certeza de la evidencia fue baja. El estudio también informó de episodios de hemorragia en el 31,7% del grupo de intervención y el 20,5% del grupo control (OR 1,8; IC del 95%: 0,96 a 3,37; evidencia de certeza baja). Estudios en curso Se encontraron 22 estudios en curso en entornos hospitalarios (20 ECA, 14 730 participantes; dos ENA, 997 participantes) en diez países diferentes (Australia [1], Brasil [1], Canadá [2], China [3], Francia [2], Alemania [1], Italia [4], Suiza [1], Reino Unido [1] y EE.UU. [6]). Doce estudios en curso tienen previsto informar sobre la mortalidad y seis tienen previsto informar sobre la asistencia respiratoria adicional. Está previsto que 13 estudios se completen en diciembre de 2020 (6959 participantes), ocho en julio de 2021 (8512 participantes) y uno en diciembre de 2021 (256 participantes). Cuatro de los estudios tienen previsto incluir 1000 participantes o más.
Conclusiones de los autores: Actualmente no hay evidencia suficiente para determinar los riesgos y los efectos beneficiosos de la profilaxis con anticoagulantes en personas hospitalizadas con covid‐19. Debido a que hay 22 estudios en curso que pretenden evaluar a más de 15 000 participantes en este entorno, se agregará evidencia más sólida a esta revisión en las actualizaciones futuras.
Trial registration: ClinicalTrials.gov NCT04354155 NCT04359212 NCT04368377 NCT04408235 NCT04344756 NCT04345848 NCT04352400 NCT04359277 NCT04360824 NCT04362085 NCT04366960 NCT04367831 NCT04372589 NCT04373707 NCT04393805 NCT04394377 NCT04397510 NCT04401293 NCT04416048.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
RLGF: none known JDST: none known PP: none known LLA: none known MC: none known MIF: none known IC: none known LS: none known CM: none known BT: none known VT: none known AA: none known LCUN: none known
Figures
References
References to studies included in this review
Ayerbe 2020 {published data only}
Liu 2020 {published data only}
-
- Liu X, Zhang X, Xiao Y, Gao T, Wang G, Wang Z, et al. Heparin-induced thrombocytopenia is associated with a high risk of mortality in critical COVID-19 patients receiving heparin-involved treatment. medRxiv [Preprint]. [DOI: 10.1101/2020.04.23.20076851] - DOI
Paranjpe 2020 {published data only}
Russo 2020 {published data only}
-
- Russo V, Di Maio M, Attena E, Silverio A, Scudiero F, Celentani D, et al. Clinical impact of pre-admission antithrombotic therapy in hospitalized patients with COVID-19: a multicenter observational study. Pharmacological Research 2020;159:104965. [DOI: 10.1016/j.phrs.2020.104965] - DOI - PMC - PubMed
Shi 2020 {published data only}
Tang 2020 {published data only}
Trinh 2020 {published data only}
-
- Trinh M, Chang DR, Govindarajulu US, Kane E, Fuster V, Kohli-Seth R, et al. Therapeutic anticoagulation is associated with decreased mortality in mechanically ventilated COVID-19 patients. medRxiv [Preprint]. [DOI: 10.1101/2020.05.30.20117929] - DOI
References to studies excluded from this review
Al‐Samkari 2020 {published data only}
Artifoni 2020 {published data only}
-
- Artifoni M, Danic G, Gautier G, Gicquel P, Boutoille D, Raffi F, et al. Systematic assessment of venous thromboembolism in COVID-19 patients receiving thromboprophylaxis: incidence and role of D-dimer as predictive factors. Journal of Thrombosis and Thrombolysis 2020;50(1):211-6. [PMID: ] - PMC - PubMed
EudraCT2020‐001823‐15 {published data only}
-
- EudraCT2020-001823-15. Evaluation of the concentration-effect relationship of enoxaparin for thromboembolic prevention in COVID-19 resuscitation patients. COV-ENOX study. clinicaltrialsregister.eu/ctr-search/trial/2020-001823-15/FR (first received 15 April 2020).
Helms 2020 {published data only}
Khider 2020 {published data only}
NCT04354155 {published data only}
-
- NCT04354155. COVID-19 anticoagulation in children - thromboprophlaxis (COVAC-TP) trial. clinicaltrials.gov/ct2/show/NCT04354155 (first received 21 April 2020).
NCT04359212 {published data only}
-
- NCT04359212. Increased risk of venous thromboembolism and higher hypercoagulable state in patients recovered in intensive care unit and in medical ward for coronavirus disease 2019 (COVID-19). clinicaltrials.gov/ct2/show/NCT04359212 (first received 21 April 2020).
NCT04365309 {published data only}
-
- NCT04365309. Protective effect of aspirin on COVID-19 patients (PEAC). clinicaltrials.gov/ct2/show/NCT04365309 (first received 28 April 2020).
NCT04368377 {published data only}
-
- NCT04368377. Platelet inhibition with GP IIb/IIIa inhibitor in critically ill patients with coronavirus disease 2019 (COVID-19). A compassionate use protocol. clinicaltrials.gov/ct2/show/NCT04368377 (first received 29 April 2020).
NCT04394000 {published data only}
-
- NCT04394000. Impact of implementation of an intensified thromboprofylaxis protocol in critically ill ICU patients with COVID-19: a longitudinal controlled before-after study. clinicaltrials.gov/ct2/show/record/NCT04394000 (first received 19 May 2020).
NCT04427098 {published data only}
-
- NCT04427098. Intermediate dose enoxaparin in hospitalized patients with moderate-severe COVID19: a pilot phase II single-arm study, INHIXACOVID19. clinicaltrials.gov/ct2/show/study/NCT04427098 (first received 11 June 2020).
Zhang 2020 {published data only}
-
- Zhang Y, Cao W, Xiao M, Li YJ, Yang Y, Zhao J, et al. Clinical and coagulation characteristics of 7 patients with critical COVID-2019 pneumonia and acro-ischemia. Zhonghua Xue Ye Xue za Zhi 2020;41(0):E006. [PMID: ] - PubMed
References to ongoing studies
ACTRN12620000517976 {published data only}
-
- ACTRN12620000517976. Can nebulised heparin reduce time to extubation in SARS CoV 2. The CHARTER study protocol. apps.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12620000517976 (first received 27 April 2020).
-
- ACTRN12620000517976p. A randomised controlled trial of nebulised heparin in critically ill mechanically ventilated patients with COVID-19 to assess the effect on the duration of mechanical ventilation. anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12620000517976 (first posted 27 April 2020).
-
- Dixon B, Smith RJ, Artigas A, Laffey J, McNicholas B, Schmidt E, et al. Can nebulised heparin reduce time to extubation in SARS CoV 2. The CHARTER study protocol. medRxiv [Preprint]. [DOI: 10.1101/2020.04.28.20082552] - DOI
ChiCTR2000030700 {published data only}
-
- ChiCTR2000030700. Study for the efficacy and safety of prolongin (enoxaparin sodium injection) in treatment of novel coronavirus pneumonia (COVID-19) adult common patients. apps.who.int/trialsearch/Trial2.aspx?TrialID=ChiCTR2000030700 (first received 10 March 2020).
-
- ChiCTR2000030700. Study for the efficacy and safety of prolongin (enoxaparin sodium injection) in treatment of novel coronavirus pneumonia (COVID-19) adult common patients. www.chictr.org.cn/showprojen.aspx?proj=50786 (first posted 10 March 2020).
ChiCTR2000030701 {published data only}
-
- ChiCTR2000030701. A randomized, parallel controlled open-label trial for the efficacy and safety of prolongin (enoxaparin sodium injection) in the treatment of adult patients with novel coronavirus pneumonia (COVID-19). chictr.org.cn/showprojen.aspx?proj=50795 (first received 10 March 2020).
ChiCTR2000030946 {published data only}
-
- ChiCTR2000030946. Effects of different VTE prevention methods on the prognosis of hospitalized patients with novel coronavirus pneumonia (COVID-19). chictr.org.cn/showprojen.aspx?proj=51265 (first received 19 March 2020).
Marietta 2020 {published data only}
-
- Marietta M, Vandelli P, Mighali P, Vicini R, Coluccio V, D'Amico R. Randomised controlled trial comparing efficacy and safety of high versus low molecular weight heparin dosages in hospitalized patients with severe COVID-19 pneumonia and coagulopathy not requiring invasive mechanical ventilation (COVID-19 HD): a structured summary of a study protocol. Trials 2020;21(1):574. [PMID: ] - PMC - PubMed
-
- NCT04408235. High versus low LMWH dosages in hospitalized patients with severe COVID-19 pneumonia and coagulopathy (COVID-19 HD). clinicaltrials.gov/ct2/show/NCT04408235 (first received 29 May 2020).
NCT04333407 {published data only}
-
- NCT04333407. Preventing cardiac complication of COVID-19 disease with early acute coronary syndrome therapy: a randomised controlled trial. clinicaltrials.gov/ct2/show/NCT04333407 (first received 3 April 2020).
NCT04344756 {published data only}
-
- NCT04344756. Trial evaluating efficacy and safety of anticoagulation in patients with COVID-19 infection, nested in the Corimmuno-19 cohort (CORIMMUNO-COAG). clinicaltrials.gov/ct2/show/study/NCT04344756 (first received 14 April 2020).
NCT04345848 {published data only}
-
- NCT04345848. Preventing COVID-19-associated thrombosis, coagulopathy and mortality with low- and high-dose anticoagulation: a randomized, open-label clinical trial. clinicaltrials.gov/ct2/show/NCT04345848 (first received 15 April 2020).
NCT04352400 {published data only}
-
- NCT04352400. Efficacy of nafamostat in COVID-19 patients (RACONA Study) (RACONA). clinicaltrials.gov/ct2/show/NCT04352400 (first posted 20 April 2020).
NCT04359277 {published data only}
-
- NCT04359277. A randomized trial of anticoagulation strategies in COVID-19. clinicaltrials.gov/ct2/show/NCT04359277 (first received 24 April 2020).
NCT04360824 {published data only}
-
- NCT04360824. COVID-19-associated coagulopathy: safety and efficacy of prophylactic anticoagulation therapy in hospitalized adults with COVID-19. clinicaltrials.gov/ct2/show/NCT04360824 (first received 24 April 2020).
NCT04362085 {published data only}
-
- NCT04362085. Coagulopathy of COVID-19: a pragmatic randomized controlled trial of therapeutic anticoagulation versus standard care as a rapid response to the COVID-19 pandemic (RAPID COVID COAG). clinicaltrials.gov/ct2/show/NCT04362085 (first received 24 April 2020).
NCT04366960 {published data only}
-
- NCT04366960. Comparison of two doses of enoxaparin for thromboprophylaxis in hospitalized COVID-19 patients. clinicaltrials.gov/ct2/show/NCT04366960 (first posted 29 April 2020).
NCT04367831 {published data only}
-
- NCT04367831. Intermediate or prophylactic-dose anticoagulation for venous or arterial thromboembolism in severe COVID-19: a cluster based randomized selection trial (IMPROVE-COVID). clinicaltrials.gov/ct2/show/NCT04367831 (first received 27 April 2020).
NCT04372589 {published data only}
-
- NCT04372589. Antithrombotic therapy to ameliorate complications of COVID-19. clinicaltrials.gov/ct2/show/NCT04372589 (first received 4 May 2020).
NCT04373707 {published data only}
-
- NCT04373707. Effectiveness of weight-adjusted prophylactic low molecular weight heparin doses compared with lower fixed prophylactic doses to prevent venous thromboembolism in COVID-2019. The multicenter randomized controlled open-label trial COVI-DOSE. clinicaltrials.gov/ct2/show/record/NCT04373707 (first received 4 May 2020).
NCT04377997 {published data only}
-
- NCT04377997. A randomized, open-label trial of therapeutic anticoagulation in COVID-19 patients with an elevated D-dimer. clinicaltrials.gov/ct2/show/NCT04377997 (first received 7 May 2020).
NCT04393805 {published data only}
-
- NCT04393805. Heparins for thromboprophylaxis in COVID-19 patients: HETHICO study in Veneto. clinicaltrials.gov/ct2/show/NCT04393805 (first received 16 May 2020).
NCT04394377 {published data only}
-
- NCT04394377. Randomized clinical trial to evaluate a routine full anticoagulation strategy in patients with coronavirus (COVID-19) - COALIZAO ACTION Trial. clinicaltrials.gov/ct2/show/NCT04394377 (first received 8 May 2020).
NCT04397510 {published data only}
-
- NCT04397510. Nebulized heparin vs. placebo for the treatment of COVID-19 induced lung injury. clinicaltrials.gov/ct2/show/NCT04397510 (first received 21 May 2020).
NCT04401293 {published data only}
-
- NCT04401293. Systemic anticoagulation with full dose low molecular weight heparin (LMWH) vs. prophylactic or intermediate dose LMWH in high risk COVID-19 patients (HEP-COVID Trial). clinicaltrials.gov/ct2/show/NCT04401293 (first received 26 May 2020).
NCT04416048 {published data only}
-
- NCT04416048. Effect of anticoagulation therapy on clinical outcomes in moderate to severe coronavirus disease 2019 (COVID-19). clinicaltrials.gov/ct2/show/NCT04416048 (first received 4 June 2020).
Additional references
Ackermann 2020
Alquwaizani 2013
Amaral 2020
AVF 2020
-
- American Venous Forum. Considerations in prophylaxis and treatment of VTE in COVID-19 patients. www.veinforum.org/wp-content/uploads/2020/04/COVID-19-White-Paper-04-17-... (accessed 3 July 2020).
Becker 2020
Biagioni 2020
-
- Biagioni RB, Lopes RD, Agati LB, Sacilotto R, Wolosker N, Sobreira ML, et al. Rationale and design for the study apixaban versus clopidogrel on a background of aspirin in patients undergoing infrapopliteal angioplasty for critical limb ischemia: AGRIPPA trial. American Heart Journal 2020;227:100-6. [DOI: 10.1016/j.ahj.2020.06.010] - DOI - PubMed
Bikdeli 2020
-
- Bikdeli B, Madhavan M, Jimenez D, Chuich T, Dreyfus I, Driggin E, et al. COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state of the art review. Journal of American College of Cardiology 2020;75(23):2950-73. [DOI: 10.1016/j.jacc.2020.04.031] - DOI - PMC - PubMed
Bilaloglu 2020
Clezar 2020
COMET 2020
-
- Core outcome set developers’ response to COVID-19 (7th July 2020). comet-initiative.org/Studies/Details/1538 (accessed 04 August 2020).
Covidence [Computer program]
-
- Veritas Health Innovation Covidence. Version accessed 1 August 2020. Melbourne, Australia: Veritas Health Innovation. Available at www.covidence.org.
Deeks 2020
-
- Deeks JJ, Higgins JP, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
Dolhnikoff 2020
Fox 2020
Giannis 2020
GRADEpro GDT 2015 [Computer program]
-
- McMaster University (developed by Evidence Prime) GRADEpro GDT. Version version accessed 1 August 2020. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Higgins 2003
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Higgins 2020a
-
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
Higgins 2020b
-
- Higgins JP, Eldridge S, Li T, editor(s). Chapter 23: Including variants on randomized trials. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
Klok 2020a
Klok 2020b
Lai 2020
-
- Lai CC, Wang CY, Wang YH, Hsueh SC, Ko WC, Hsueh PR. Global epidemiology of coronavirus disease 2019 (COVID-19): disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status. International Journal of Antimicrobial Agents 2020;55(4):105946. [PMID: ] - PMC - PubMed
Lefebvre 2020
-
- Lefebvre C, Glanville J, Briscoe S, Littlewood A, Marshall C, Metzendorf M-I, et al. Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020). Cochrane, 2020. Available from www.training.cochrane.org/handbook.
Li 2020
Liberati 2009
Liu 2019
-
- Liu Y, Mu S, Li X, Liang Y, Wang L, Ma X. Unfractionated heparin alleviates sepsis-induced acute lung injury by protecting tight junctions. Journal of Surgical Research 2019;238:175-85. [PMID: ] - PubMed
Long 2020
Marini 2020
McGuinness 2020
NHS 2020
-
- NHS England and NHS Improvement. Clinical guide for the management of anticoagulant services during the coronavirus pandemic. www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0077... (accessed 3 July 2020).
Obe 2020
-
- Obe BH, Retter A, McClintock C. Practical guidance for the prevention of thrombosis and management of coagulopathy and disseminated intravascular coagulation of patients infected with COVID-19. thrombosisuk.org/downloads/T&H%20and%20COVID.pdf (accessed 3 July 2020).
Oxley 2020
Pang 2020
Panigada 2020
-
- Panigada M, Bottino N, Tagliabue P, Grasselli G, Novembrino C, Chantarangkul V, et al. Hypercoagulability of COVID-19 patients in intensive care unit: a report of thromboelastography findings and other parameters of hemostasis. Journal of Thrombosis and Haemostasis 2020;18(7):1738-42. [PMID: ] - PMC - PubMed
Poston 2020
Ramacciotti 2020
Review Manager 2020 [Computer program]
-
- The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.4. Copenhagen: The Cochrane Collaboration, 2020.
Robvis [Computer program]
-
- Robvis (visualization tool). Version accessed 20 August 2020. Bristol, UK: Luke McGuinness. Available at mcguinlu.shinyapps.io/robvis/.
Sanders 2020
Schulman 2010
-
- Schulman S, Angerås U, Bergqvist D, Eriksson B, Lassen MR, Fisher W. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. Journal of Thrombosis and Haemostasis : JTH 2010;8(1):202-4. [PMID: ] - PubMed
Schünemann 2013
-
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.gradepro.org/app/handbook/handbook.html.
Schünemann 2019
-
- Schünemann HJ, Vist GE, Higgins JP, Santesso N, Deeks JJ, Glasziou P, et al. Chapter 15: Interpreting results and drawing conclusions. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from www.training.cochrane.org/handbook.
Sterne 2016
Tobaiqy 2020
Violi 2020
Wan 2014
Ware 1992
-
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care 1992;30(6):473-83. [PMID: ] - PubMed
Young 2008
-
- Young E. The anti-inflammatory effects of heparin and related compounds. Thrombosis Research 2008;122(6):743-52. [PMID: ] - PubMed
References to other published versions of this review
Flumignan 2020
-
- Flumignan RL, Tinôco JD, Pascoal PI, Areias LL, Cossi MS, Fernandes MI et al. Prophylactic anticoagulants for patients hospitalised with COVID-19 (Protocol). available from doi.org/10.17605/OSF.IO/8PRXW (registered 7 August 2020).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous