

Digital Pathology During the COVID-19 Outbreak in Italy: Survey Study
- PMID: 33503002
- PMCID: PMC7901595
- DOI: 10.2196/24266
Digital Pathology During the COVID-19 Outbreak in Italy: Survey Study
Abstract
Background: Transition to digital pathology usually takes months or years to be completed. We were familiarizing ourselves with digital pathology solutions at the time when the COVID-19 outbreak forced us to embark on an abrupt transition to digital pathology.
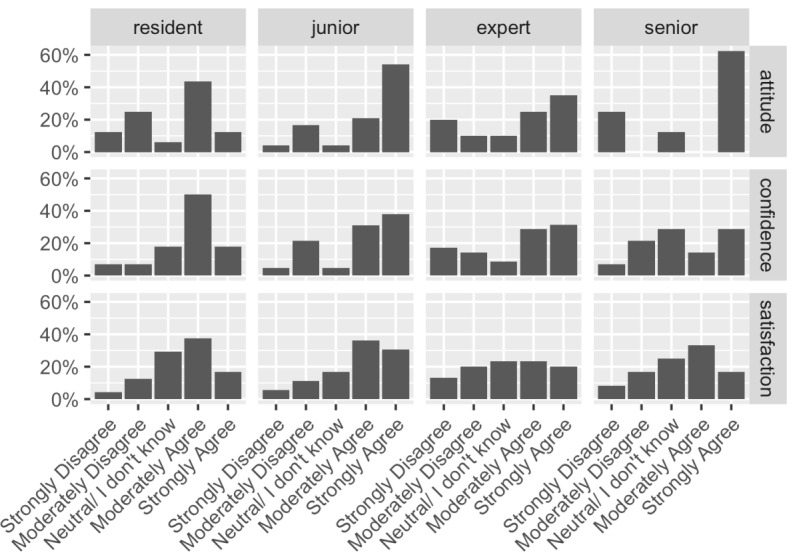
Objective: The aim of this study was to quantitatively describe how the abrupt transition to digital pathology might affect the quality of diagnoses, model possible causes by probabilistic modeling, and qualitatively gauge the perception of this abrupt transition.
Methods: A total of 17 pathologists and residents participated in this study; these participants reviewed 25 additional test cases from the archives and completed a final psychologic survey. For each case, participants performed several different diagnostic tasks, and their results were recorded and compared with the original diagnoses performed using the gold standard method (ie, conventional microscopy). We performed Bayesian data analysis with probabilistic modeling.
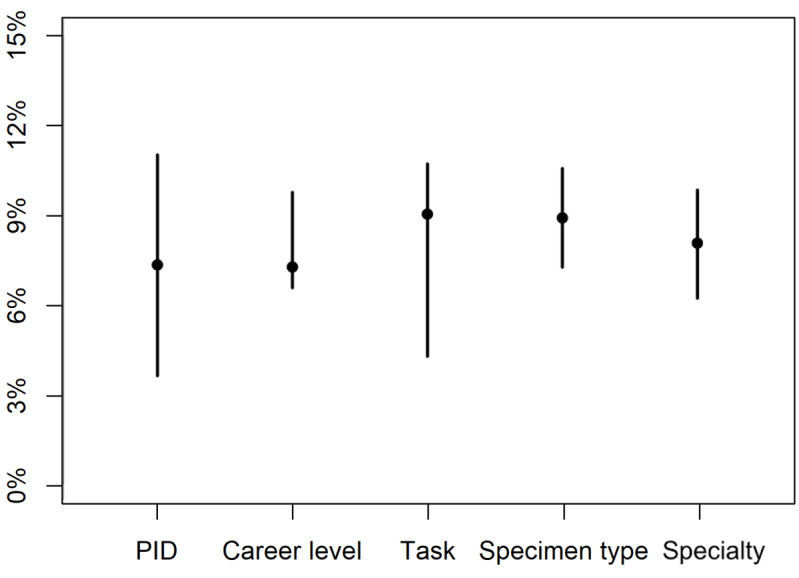
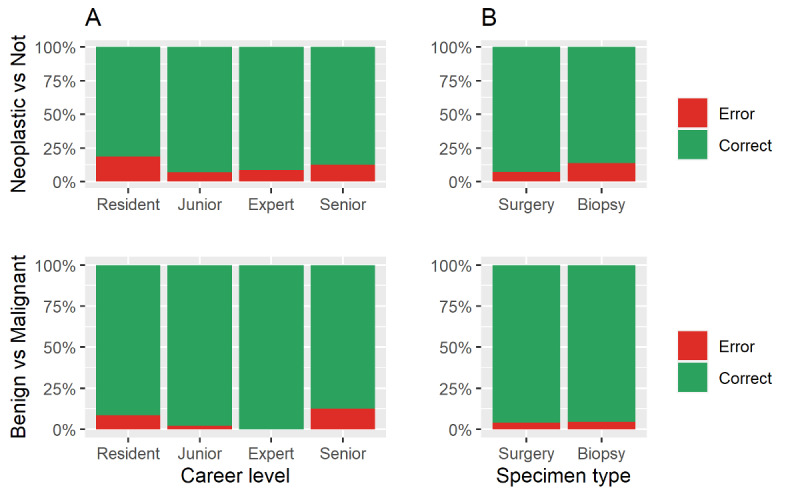
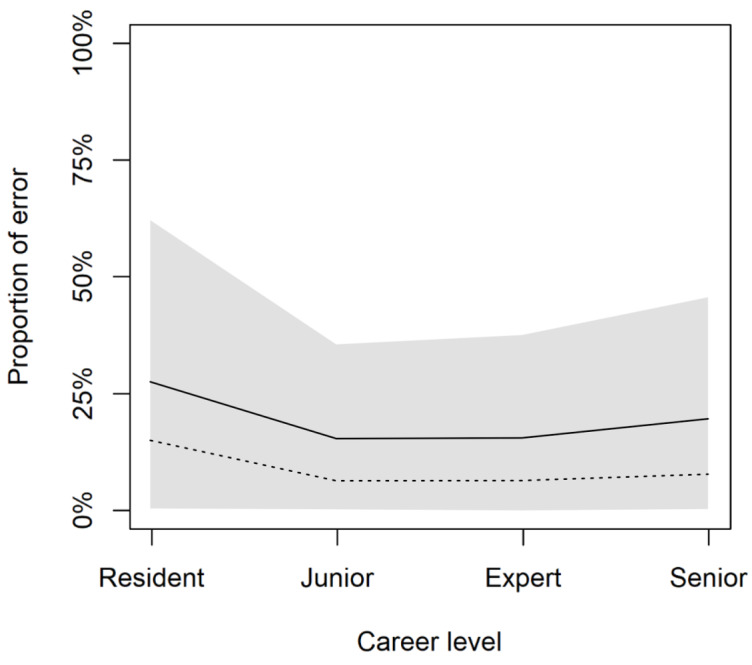
Results: The overall analysis, comprising 1345 different items, resulted in a 9% (117/1345) error rate in using digital slides. The task of differentiating a neoplastic process from a nonneoplastic one accounted for an error rate of 10.7% (42/392), whereas the distinction of a malignant process from a benign one accounted for an error rate of 4.2% (11/258). Apart from residents, senior pathologists generated most discrepancies (7.9%, 13/164). Our model showed that these differences among career levels persisted even after adjusting for other factors.
Conclusions: Our findings are in line with previous findings, emphasizing that the duration of transition (ie, lengthy or abrupt) might not influence the diagnostic performance. Moreover, our findings highlight that senior pathologists may be limited by a digital gap, which may negatively affect their performance with digital pathology. These results can guide the process of digital transition in the field of pathology.
Keywords: Bayesian data analysis; COVID19; digital pathology; probabilistic modeling.
©Simone Giaretto, Salvatore Lorenzo Renne, Daoud Rahal, Paola Bossi, Piergiuseppe Colombo, Paola Spaggiari, Sofia Manara, Mauro Sollai, Barbara Fiamengo, Tatiana Brambilla, Bethania Fernandes, Stefania Rao, Abubaker Elamin, Marina Valeri, Camilla De Carlo, Vincenzo Belsito, Cesare Lancellotti, Miriam Cieri, Angelo Cagini, Luigi Terracciano, Massimo Roncalli, Luca Di Tommaso. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 22.02.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Pantanowitz L, Sharma A, Carter A, Kurc T, Sussman A, Saltz J. Twenty years of digital pathology: an overview of the road travelled, what is on the horizon, and the emergence of vendor-neutral archives. J Pathol Inform. 2018;9:40. doi: 10.4103/jpi.jpi_69_18. http://www.jpathinformatics.org/article.asp?issn=2153-3539;year=2018;vol... - DOI - PMC - PubMed
-
- Hartman D, Pantanowitz L, McHugh J, Piccoli A, OLeary M, Lauro G. Enterprise implementation of digital pathology: feasibility, challenges, and opportunities. J Digit Imaging. 2017 Oct;30(5):555–560. doi: 10.1007/s10278-017-9946-9. http://europepmc.org/abstract/MED/28116576 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
