

Factors associated with actively working in the very long-term following acute coronary syndrome
- PMID: 33503196
- PMCID: PMC7811831
- DOI: 10.6061/clinics/2021/e2553
Factors associated with actively working in the very long-term following acute coronary syndrome
Abstract
Objectives: Returning to work after an episode of acute coronary syndrome (ACS) is challenging for many patients, and has both personal and social impacts. There are limited data regarding the working status in the very long-term after ACS.
Methods: We retrospectively analyzed 1,632 patients who were working prior to hospitalization for ACS in a quaternary hospital and were followed-up for up to 17 years. Adjusted models were developed to analyze the variables independently associated with actively working at the last contact, and a prognostic predictive index for not working at follow-up was developed.
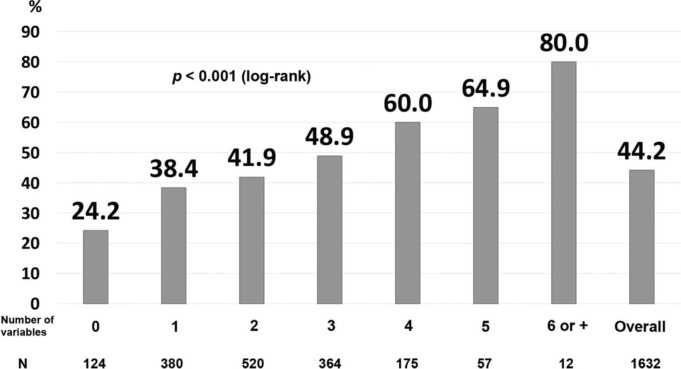
Results: The following variables were significantly and independently associated with actively working at the last contact: age>median (hazard-ratio [HR], 0.76, p<0.001); male sex (HR, 1.52, p<0.001); government health insurance (HR, 1.36, p<0.001); history of angina (HR, 0.69, p<0.001) or myocardial infarction (MI) (HR, 0.76, p=0.005); smoking (HR, 0.81, p=0.015); ST-elevation MI (HR, 0.81, p=0.021); anterior-wall MI (HR, 0.75, p=0.001); non-primary percutaneous coronary intervention (PCI) (HR, 0.77, p=0.002); fibrinolysis (HR, 0.61, p<0.001); cardiogenic shock (HR, 0.60, p=0.023); statin (HR, 3.01, p<0.001), beta-blocker (HR, 1.26, p=0.020), angiotensin-converting enzyme (ACE) inhibitor/angiotensin II receptor blocker (ARB) (HR, 1.37, p=0.001) at hospital discharge; and MI at follow-up (HR, 0.72, p=0.001). The probability of not working at the last contact ranged from 24.2% for patients with no variables, up to 80% for patients with six or more variables.
Conclusions: In patients discharged after ACS, prior and in-hospital clinical variables, as well as the quality of care at discharge, have a great impact on the long-term probability of actively working.
Conflict of interest statement
No potential conflict of interest was reported.
Figures


References
-
- World Health Organization . The Global Burden of Disease: 2016 update. [cited January 15th, 2020] Available from: http://www.who.int/evidence/bod.
-
- GBD 2017 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922. doi: 10.1016/S0140-6736(18)32335-3. - DOI - PMC - PubMed
-
- Schmidt M, Jacobsen JB, Lash TL, Botker HE, Sorensen HT. 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ. 2012;344:e356. doi: 10.1136/bmj.e356. - DOI - PMC - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation. 2018;137(12):e67–e492. doi: 10.1161/CIR.0000000000000558. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
