

Vascularized bone grafts for post-traumatic defects in the upper extremity
- PMID: 33503750
- PMCID: PMC7861969
- DOI: 10.5999/aps.2020.00969
Vascularized bone grafts for post-traumatic defects in the upper extremity
Abstract
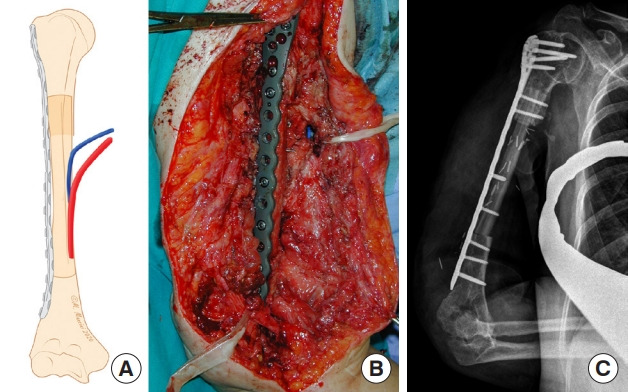
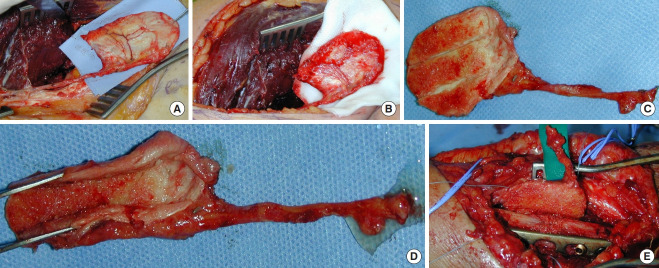
Vascularized bone grafts (VBGs) are widely employed to reconstruct upper extremity bone defects. Conventional bone grafting is generally used to treat defects smaller than 5-6 cm, when tissue vascularization is adequate and there is no infection risk. Vascularized fibular grafts (VFGs) are mainly used in the humerus, radius or ulna in cases of persistent non-union where traditional bone grafting has failed or for bone defects larger than 6 cm. Furthermore, VFGs are considered to be the standard treatment for large bone defects located in the radius, ulna and humerus and enable the reconstruction of soft-tissue loss, as VFGs can be harvested as osteocutaneous flaps. VBGs enable one-stage surgical reconstruction and are highly infection-resistant because of their autonomous vascularization. A vascularized medial femoral condyle (VFMC) free flap can be used to treat small defects and non-unions in the upper extremity. Relative contraindications to these procedures are diabetes, immunosuppression, chronic infections, alcohol, tobacco, drug abuse and obesity. The aim of our study was to illustrate the use of VFGs to treat large post-traumatic bone defects and osteomyelitis located in the upper extremity. Moreover, the use of VFMC autografts is presented.
Keywords: Bone; Cortico-periosteal; Fibula; Graft; Microsurgery.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures





References
-
- Klifto CS, Gandi SD, Sapienza A. Bone graft options in upper-extremity surgery. J Hand Surg Am. 2018;43:755–61. - PubMed
-
- Khan SN, Cammisa FP, Jr, Sandhu HS, et al. The biology of bone grafting. J Am Acad Orthop Surg. 2005;13:77–86. - PubMed
-
- Taylor GI, Miller GD, Ham FJ. The free vascularized bone graft: a clinical extension of microvascular techniques. Plast Reconstr Surg. 1975;55:533–44. - PubMed
-
- Adani R, Delcroix L, Innocenti M, et al. Reconstruction of large posttraumatic skeletal defects of the forearm by vascularized free fibular graft. Microsurgery. 2004;24:423–9. - PubMed
-
- Safoury Y. Free vascularized fibula for the treatment of traumatic bone defects and nonunion of the forearm bones. J Hand Surg Br. 2005;30:67–72. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources