

Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders
- PMID: 33503811
- PMCID: PMC7908360
- DOI: 10.3390/ijerph18031028
Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders
Abstract
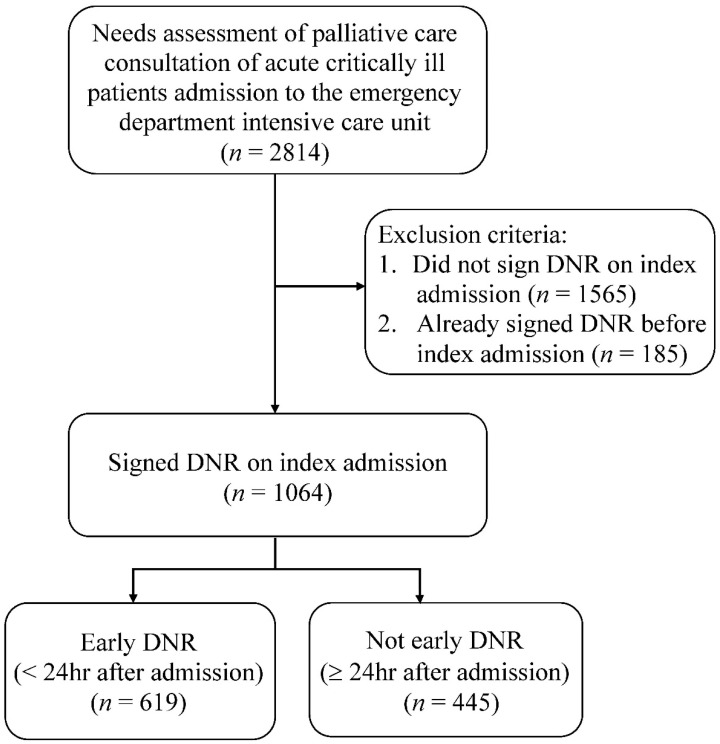
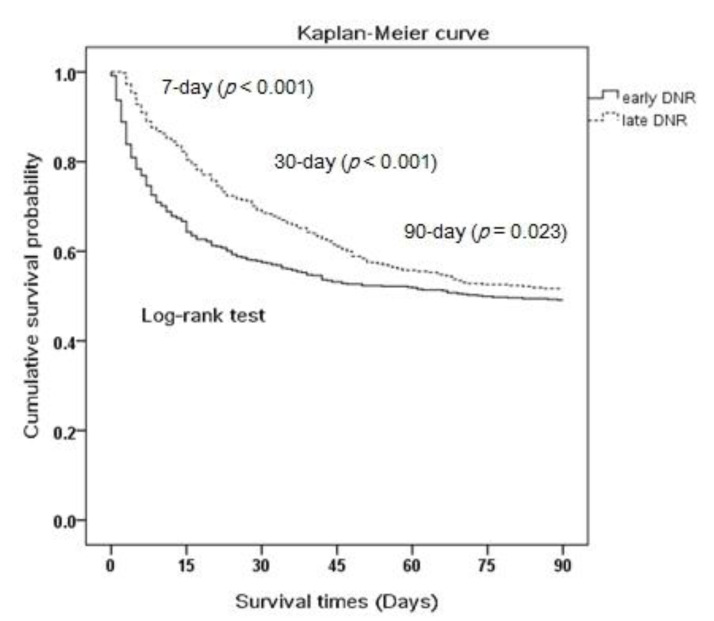
Background: A do-not-resuscitate (DNR) order is associated with an increased risk of death among emergency department (ED) patients. Little is known about patient characteristics, hospital care, and outcomes associated with the timing of the DNR order. Aim: Determine patient characteristics, hospital care, survival, and resource utilization between patients with early DNR (EDNR: signed within 24 h of ED presentation) and late DNR orders. Design: Retrospective observational study. Setting/Participants: We enrolled consecutive, acute, critically ill patients admitted to the emergency intensive care unit (EICU) at Taipei Veterans General Hospital from 1 February 2018, to 31 January 2020. Results: Of the 1064 patients admitted to the EICU, 619 (58.2%) had EDNR and 445 (41.8%) LDNR. EDNR predictors were age >85 years (adjusted odd ratios (AOR) 1.700, 1.027-2.814), living in long-term care facilities (AOR 1.880, 1.066-3.319), having advanced cardiovascular diseases (AOR 2.128, 1.039-4.358), "medical staff would not be surprised if the patient died within 12 months" (AOR 1.725, 1.193-2.496), and patients' family requesting palliative care (AOR 2.420, 1.187-4.935). EDNR patients underwent lesser endotracheal tube (ET) intubation (15.6% vs. 39.9%, p < 0.001) and had reduced epinephrine injection (19.9% vs. 30.3%, p = 0.009), ventilator support (16.7% vs. 37.9%, p < 0.001), and narcotic use (51.1% vs. 62.6%, p = 0.012). EDNR patients had significantly lower 7-day (p < 0.001), 30-day (p < 0.001), and 90-day (p = 0.023) survival. Conclusions: EDNR patients underwent decreased ET intubation and had reduced epinephrine injection, ventilator support, and narcotic use during EOL as well as decreased length of hospital stay, hospital expenditure, and survival compared to LDNR patients.
Keywords: do-not-resuscitate; emergency department; hospital care; intensive care unit.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Auerbach A.D., Katz R., Pantilat S.Z., Bernacki R., Schnipper J., Kaboli P., Wetterneck T., Gonzales D., Arora V., Zhang J., et al. Factors associated with discussion of care plans and code status at the time of hospital admission: Results from the multicenter hospitalist study. J. Hosp. Med. 2008;3:437–445. doi: 10.1002/jhm.369. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
