

Incretin Hormones in Obesity and Related Cardiometabolic Disorders: The Clinical Perspective
- PMID: 33503878
- PMCID: PMC7910956
- DOI: 10.3390/nu13020351
Incretin Hormones in Obesity and Related Cardiometabolic Disorders: The Clinical Perspective
Abstract
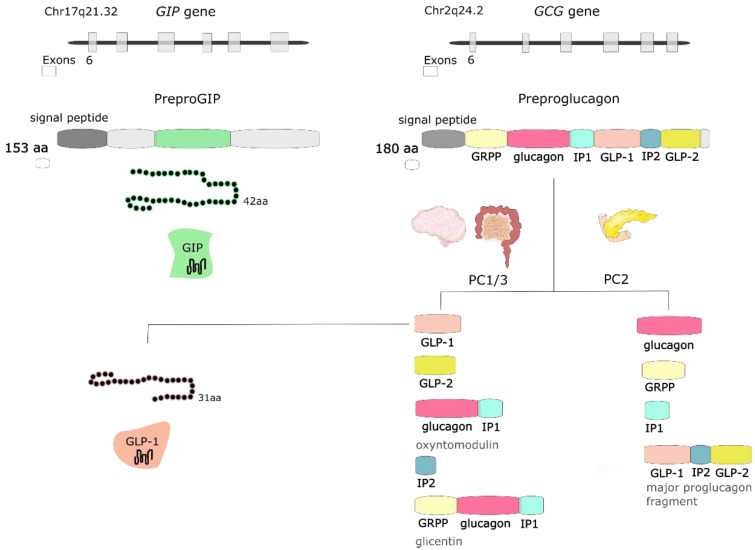
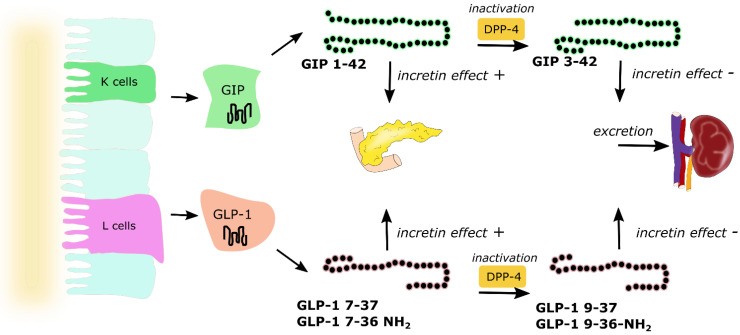
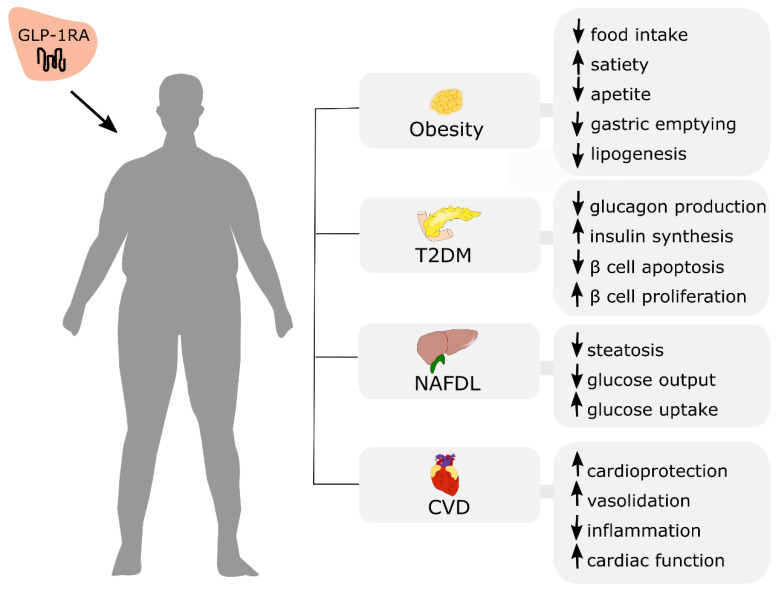
The prevalence of obesity continues to grow rapidly worldwide, posing many public health challenges of the 21st century. Obese subjects are at major risk for serious diet-related noncommunicable diseases, including type 2 diabetes mellitus, cardiovascular disease, and non-alcoholic fatty liver disease. Understanding the mechanisms underlying obesity pathogenesis is needed for the development of effective treatment strategies. Dysregulation of incretin secretion and actions has been observed in obesity and related metabolic disorders; therefore, incretin-based therapies have been developed to provide new therapeutic options. Incretin mimetics present glucose-lowering properties, together with a reduction of appetite and food intake, resulting in weight loss. In this review, we describe the physiology of two known incretins-glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1), and their role in obesity and related cardiometabolic disorders. We also focus on the available and incoming incretin-based medications that can be used in the treatment of the above-mentioned conditions.
Keywords: GIP; GLP-1; cardiovascular disease; incretin-based therapy; incretins; non-alcoholic fatty liver disease; obesity; type 2 diabetes mellitus.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
The influence of Glucose-dependent Insulinotropic Polypeptide (GIP) on human adipose tissue and fat metabolism: Implications for obesity, type 2 diabetes and Non-Alcoholic Fatty Liver Disease (NAFLD).Peptides. 2020 Mar;125:170208. doi: 10.1016/j.peptides.2019.170208. Epub 2019 Nov 20. Peptides. 2020. PMID: 31759125 Review.
-
Physiology of incretins and loss of incretin effect in type 2 diabetes and obesity.Arch Physiol Biochem. 2013 Oct;119(4):170-8. doi: 10.3109/13813455.2013.812664. Epub 2013 Jul 16. Arch Physiol Biochem. 2013. PMID: 23859800 Review.
-
Incretin hormones: Their role in health and disease.Diabetes Obes Metab. 2018 Feb;20 Suppl 1:5-21. doi: 10.1111/dom.13129. Diabetes Obes Metab. 2018. PMID: 29364588 Review.
-
Incretins in obesity and diabetes.Ann N Y Acad Sci. 2020 Feb;1461(1):104-126. doi: 10.1111/nyas.14211. Epub 2019 Aug 7. Ann N Y Acad Sci. 2020. PMID: 31392745 Free PMC article. Review.
-
Physiology of incretins in health and disease.Rev Diabet Stud. 2011 Fall;8(3):293-306. doi: 10.1900/RDS.2011.8.293. Epub 2011 Nov 10. Rev Diabet Stud. 2011. PMID: 22262068 Free PMC article. Review.
Cited by
-
Obesity and Type 2 Diabetes: Adiposopathy as a Triggering Factor and Therapeutic Options.Molecules. 2023 Mar 30;28(7):3094. doi: 10.3390/molecules28073094. Molecules. 2023. PMID: 37049856 Free PMC article. Review.
-
The interplay of oxytocin and dopaminergic system: Effects on food consumption in broiler chickens.Poult Sci. 2025 Jun;104(6):105139. doi: 10.1016/j.psj.2025.105139. Epub 2025 Apr 3. Poult Sci. 2025. PMID: 40199125 Free PMC article.
-
Curbing the Obesity Epidemic: Should GLP-1 Receptor Agonists Be the Standard of Care for Obesity?Curr Cardiol Rep. 2024 Sep;26(9):1011-1019. doi: 10.1007/s11886-024-02097-4. Epub 2024 Jul 20. Curr Cardiol Rep. 2024. PMID: 39031282 Review.
-
Glucagon-like peptide-1: a multi-faceted anti-inflammatory agent.Front Immunol. 2023 May 17;14:1148209. doi: 10.3389/fimmu.2023.1148209. eCollection 2023. Front Immunol. 2023. PMID: 37266425 Free PMC article. Review.
-
Effect of nipa palm (Nypa fruticans Wurmb.) vinegar on the incretin hormones and intestinal glucose transporters in type 2 diabetes mellitus rat model.BMC Complement Med Ther. 2025 May 30;25(1):192. doi: 10.1186/s12906-025-04933-8. BMC Complement Med Ther. 2025. PMID: 40448078 Free PMC article.
References
-
- WHO Website Fact Sheets: Obesity and Overweight. [(accessed on 22 December 2020)]; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
-
- OECD . The Heavy Burden of Obesity: The Economics of Prevention. OECD Publishing; Paris, France: 2019. OECD Health Policy Studies.
-
- Finer N. Medical consequences of obesity. Medicine. 2015;43:88–93. doi: 10.1016/j.mpmed.2014.11.003. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
