

Acute Imaging Findings Predict Recovery of Cognitive and Motor Function after Inpatient Rehabilitation for Pediatric Traumatic Brain Injury: A Pediatric Brain Injury Consortium Study
- PMID: 33504256
- PMCID: PMC8418527
- DOI: 10.1089/neu.2020.7437
Acute Imaging Findings Predict Recovery of Cognitive and Motor Function after Inpatient Rehabilitation for Pediatric Traumatic Brain Injury: A Pediatric Brain Injury Consortium Study
Abstract
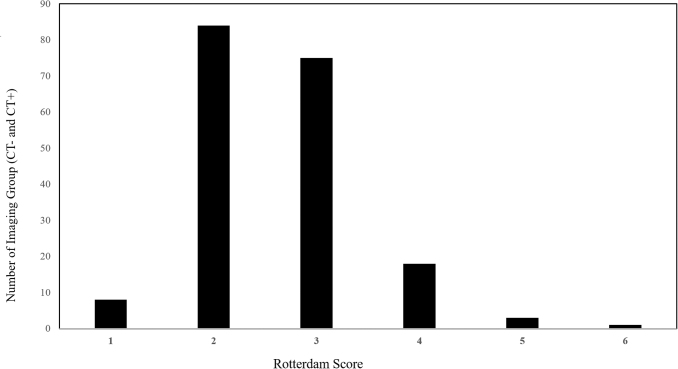
Traumatic brain injury (TBI) is a major cause of morbidity and mortality in children; survivors experience long-term cognitive and motor deficits. To date, studies predicting outcome following pediatric TBI have primarily focused on acute behavioral responses and proxy measures of injury severity; unsurprisingly, these measures explain very little of the variance following heterogenous injury. In adults, certain acute imaging biomarkers help predict cognitive and motor recovery following moderate to severe TBI. This multi-center, retrospective study, characterizes the day-of-injury computed tomographic (CT) reports of pediatric, adolescent, and young adult patients (2 months to 21 years old) who received inpatient rehabilitation services for TBI (n = 247). The study also determines the prognostic utility of CT findings for cognitive and motor outcomes assessed by the Pediatric Functional Independence Measure, converted to age-appropriate developmental functional quotient (DFQ), at discharge from rehabilitation. Subdural hematomas (66%), contusions (63%), and subarachnoid hemorrhages (59%) were the most common lesions; the majority of subjects had less severe Rotterdam CT scores (88%, ≤ 3). After controlling for age, gender, mechanism of injury, length of acute hospital stay, and admission DFQ in multivariate regression analyses, the highest Rotterdam score (β = -25.2, p < 0.01) and complete cisternal effacement (β = -19.4, p < 0.05) were associated with lower motor DFQ, and intraventricular hemorrhage was associated with lower motor (β = -3.7, p < 0.05) and cognitive DFQ (β = -4.9, p < 0.05). These results suggest that direct detection of intracranial injury provides valuable information to aid in prediction of recovery after pediatric TBI, and needs to be accounted for in future studies of prognosis and intervention.
Keywords: Rotterdam criteria; WeeFIM; computed tomography; pediatric traumatic brain injury; rehabilitation.
Conflict of interest statement
No competing financial interests exist.
Figures

References
-
- Keenan, H.T., and Bratton, S.L. (2006). Epidemiology and outcomes of pediatric traumatic brain injury. Dev. Neurosci. 28, 256–263 - PubMed
-
- Kochanek, P.M., Tasker, R.C., Bell, M.J., Adelson, P.D., Carney, N., Vavilala, M.S., Selden, N.R., Bratton, S.L., Grant, G.A., Kissoon, N., Reuter-Rice, K.E., and Wainwright, M.S. (2019). Management of pediatric severe traumatic brain injury: 2019 consensus and guidelines-based algorithm for first and second tier therapies. Pediatr. Crit. Care Med. 20, 269–279 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
