

Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry
- PMID: 33504483
- PMCID: PMC7843211
- DOI: 10.1136/annrheumdis-2020-219498
Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry
Abstract
Objectives: To determine factors associated with COVID-19-related death in people with rheumatic diseases.
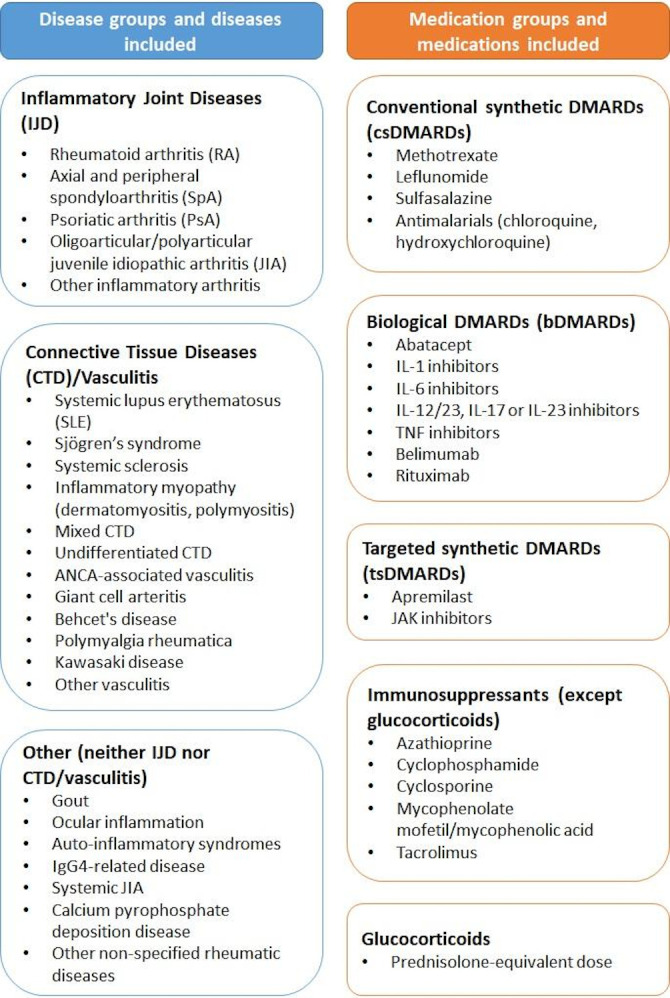
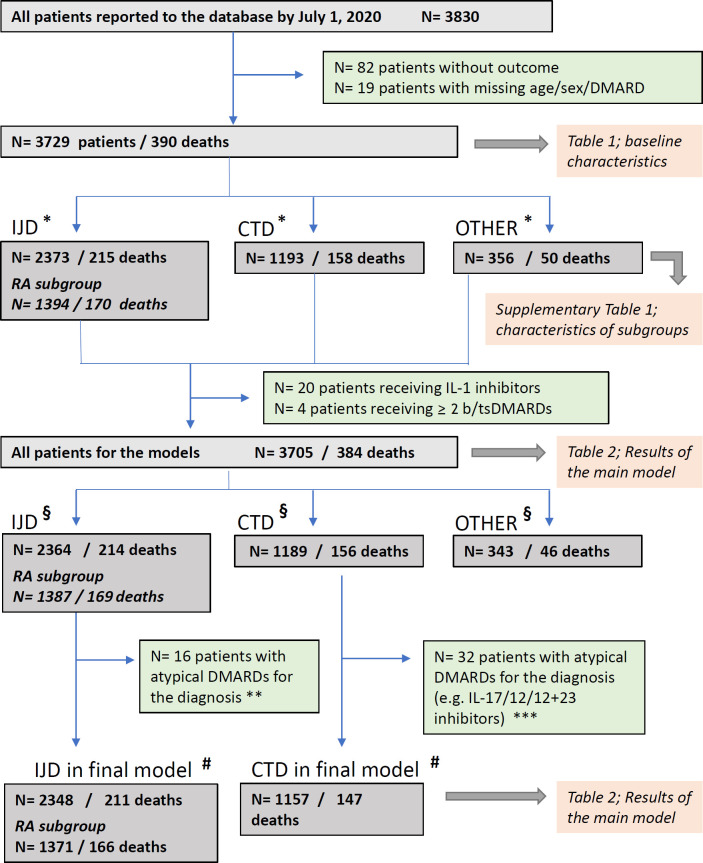
Methods: Physician-reported registry of adults with rheumatic disease and confirmed or presumptive COVID-19 (from 24 March to 1 July 2020). The primary outcome was COVID-19-related death. Age, sex, smoking status, comorbidities, rheumatic disease diagnosis, disease activity and medications were included as covariates in multivariable logistic regression models. Analyses were further stratified according to rheumatic disease category.
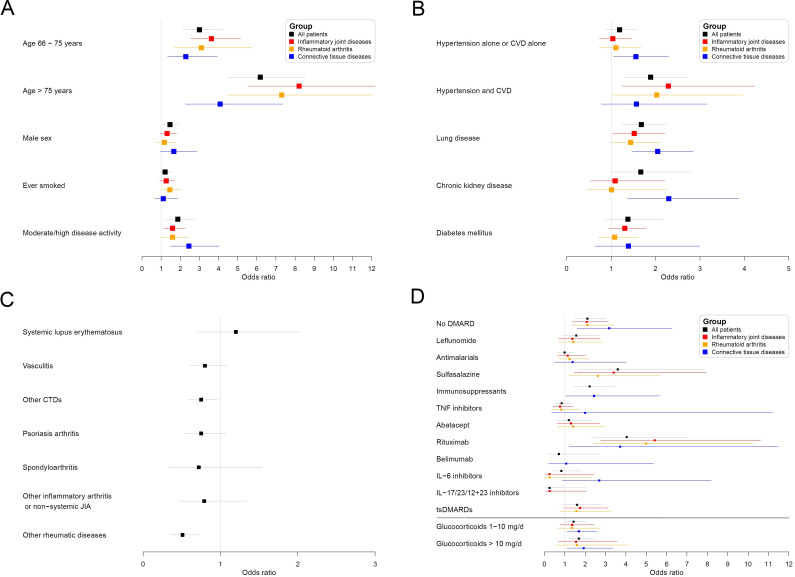
Results: Of 3729 patients (mean age 57 years, 68% female), 390 (10.5%) died. Independent factors associated with COVID-19-related death were age (66-75 years: OR 3.00, 95% CI 2.13 to 4.22; >75 years: 6.18, 4.47 to 8.53; both vs ≤65 years), male sex (1.46, 1.11 to 1.91), hypertension combined with cardiovascular disease (1.89, 1.31 to 2.73), chronic lung disease (1.68, 1.26 to 2.25) and prednisolone-equivalent dosage >10 mg/day (1.69, 1.18 to 2.41; vs no glucocorticoid intake). Moderate/high disease activity (vs remission/low disease activity) was associated with higher odds of death (1.87, 1.27 to 2.77). Rituximab (4.04, 2.32 to 7.03), sulfasalazine (3.60, 1.66 to 7.78), immunosuppressants (azathioprine, cyclophosphamide, ciclosporin, mycophenolate or tacrolimus: 2.22, 1.43 to 3.46) and not receiving any disease-modifying anti-rheumatic drug (DMARD) (2.11, 1.48 to 3.01) were associated with higher odds of death, compared with methotrexate monotherapy. Other synthetic/biological DMARDs were not associated with COVID-19-related death.
Conclusion: Among people with rheumatic disease, COVID-19-related death was associated with known general factors (older age, male sex and specific comorbidities) and disease-specific factors (disease activity and specific medications). The association with moderate/high disease activity highlights the importance of adequate disease control with DMARDs, preferably without increasing glucocorticoid dosages. Caution may be required with rituximab, sulfasalazine and some immunosuppressants.
Keywords: antirheumatic agents; autoimmune diseases; epidemiology; glucocorticoids; health care; outcome assessment.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AS reports personal fees from lectures for AbbVie, MSD, Roche, BMS and Pfizer, all outside the submitted work. MG reports grants from National Institutes of Health, NIAMS, outside the submitted work. JL reports a research grant from Pfizer, outside of the submitted work. EFM reports that LPCDR received support for specific activities: grants from Abbvie, Novartis, Janssen-Cilag, Lilly Portugal, Sanofi, Grünenthal S.A., MSD, Celgene, Medac, Pharmakern and GAfPA; grants and non-financial support from Pfizer; non-financial support from Grünenthal GmbH, outside the submitted work. CR has received consulting/speaker’s fees from Abbvie, Amgen, AstraZeneca, BMS, Biogen, Eli Lilly, Glenmark, GSK, MSD, Mylan and Pfizer, and grants from Biogen, Lilly and Nordic Pharma, all unrelated to this manuscript. MJS is supported by unrestricted grants from AbbVie, Biogen, Gilead, Lilly, MSD, Novartis and Pfizer. Her work is supported by grants from the National Institutes of Health and Agency for Healthcare Research and Quality. She leads the Data Analytic Center for the American College of Rheumatology, which is unrelated to this work. ES reports non-financial support from Canadian Arthritis Patient Alliance, outside the submitted work. JS is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (grant numbers K23 AR069688, R03 AR075886, L30 AR066953, P30 AR070253 and P30 AR072577), the Rheumatology Research Foundation (R Bridge Award), the Brigham Research Institute, and the R. Bruce and Joan M. Mickey Research Scholar Fund. He has received research support from Amgen and Bristol-Myers Squibb and performed consultancy for Bristol-Myers Squibb, Gilead, Inova Diagnostics, Janssen, Optum and Pfizer unrelated to this work. PS reports personal fees from American College of Rheumatology/Wiley Publishing, outside the submitted work. TT reports personal fees for lectures and expertises from Amgen, Arrow, Biogen, BMS, Chugai, Expanscience, Gilead, Grunenthal, LCA, Lilly, Medac, MSD, Nordic, Novartis, Pfizer, Sandoz, Sanofi, Theramex, Thuasne, TEVA and UCB, and reports financial support or fees for research activities from Amgen, Bone Therapeutics, Chugai, MSD, Novartis, Pfizer and UCB, all unrelated to this manuscript. ZSW reports grant support from Bristol-Myers Squibb and consulting fees from Viela Bio. JB-C has received consulting/speaker’s fees from Abbvie, MSD, BMS and Roche, and grants from Pfizer, all unrelated to this manuscript. He reports non-branded marketing campaigns for Novartis. PC has received consulting and lecturing fees from Abbvie, AstraZeneca, Bristol-Myers Squibb, Gilead, Glaxo Smith Kline, Innotech, Janssen, Merck Sharp Dohme, Roche, Servier and Vifor. LC has not received fees or personal grants from any laboratory, but her institute works by contract for laboratories among other institutions, such as Abbvie Spain, Eisai, Gebro Pharma, Merck Sharp & Dohme España, S.A., Novartis Farmaceutica, Pfizer, Roche Farma, Sanofi Aventis, Astellas Pharma, Actelion Pharmaceuticals España, Grünenthal GmbH and UCB Pharma. LG reports personal consultant fees from AbbVie, Amgen, BMS, Biogen, Celgene, Gilead, Janssen, Lilly, Novartis, Pfizer, Samsung Bioepis, Sanofi-Aventis and UCB, and grants from Amgen, Lilly, Janssen, Pfizer, Sandoz, Sanofi and Galapagos, all unrelated to this manuscript. RG reports non-financial support from Pfizer Australia, personal fees from Pfizer Australia, personal fees from Cornerstones, personal fees from Janssen New Zealand, non-financial support from Janssen Australia, personal fees from Novartis, outside the submitted work. EH reports personal consultant fees from Actelion, Sanofi-Genzyme and GSK, and grants from GSK, all unrelated to this manuscript. RH reports research grant from Pfizer and personal fees from AbbVie, Pfizer, Novartis, Amgen, Mylan, Gilead, Medac and Takeda, all outside the submitted work. JH reports grants from Rheumatology Research Foundation, grants from Childhood Arthritis and Rheumatology Research Alliance (CARRA), personal fees from Novartis, outside the submitted work. KLH reports she has received non-personal speaker’s fees from Abbvie and grant income from BMS, UCB and Pfizer, all unrelated to this manuscript. KLH is supported by the NIHR Manchester Biomedical Research Centre. PCR reports personal fees from Abbvie, Eli Lilly, Gilead, Janssen, Novartis, Pfizer, Roche and UCB, non-financial support from BMS, research funding from Janssen, Novartis, Pfizer and UCB, all outside the submitted work. JY reports consulting fees from AstraZeneca and Eli Lilly, and grants from Pfizer, outside the submitted work. PMM has received consulting/speaker’s fees from Abbvie, BMS, Celgene, Eli Lilly, Janssen, MSD, Novartis, Orphazyme, Pfizer, Roche and UCB, all unrelated to this manuscript, and is supported by the National Institute for Health Research (NIHR), University College London Hospitals (UCLH) and Biomedical Research Centre (BRC).
Figures
Comment in
-
Response to: 'Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician reported registry' by Arnaud and Devilliers.Ann Rheum Dis. 2023 May;82(5):e114. doi: 10.1136/annrheumdis-2021-220058. Epub 2021 Feb 18. Ann Rheum Dis. 2023. PMID: 33602795 No abstract available.
-
Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry'.Ann Rheum Dis. 2023 May;82(5):e113. doi: 10.1136/annrheumdis-2021-220037. Epub 2021 Feb 18. Ann Rheum Dis. 2023. PMID: 33602796 No abstract available.
-
Timing of rituximab and immunoglobulin level influence the risk of death for COVID-19 in ANCA-associated vasculitis.Rheumatology (Oxford). 2021 Jul 1;60(7):3476-3477. doi: 10.1093/rheumatology/keab175. Rheumatology (Oxford). 2021. PMID: 33609106 Free PMC article. No abstract available.
-
Response to: 'Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician reported registry'' by Mulhearn et al.Ann Rheum Dis. 2023 May;82(5):e116. doi: 10.1136/annrheumdis-2021-220134. Epub 2021 Mar 1. Ann Rheum Dis. 2023. PMID: 33648957 No abstract available.
-
Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry'.Ann Rheum Dis. 2023 May;82(5):e115. doi: 10.1136/annrheumdis-2021-220099. Epub 2021 Mar 1. Ann Rheum Dis. 2023. PMID: 33648958 No abstract available.
-
Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry'.Ann Rheum Dis. 2023 Jun;82(6):e138. doi: 10.1136/annrheumdis-2021-220588. Epub 2021 May 13. Ann Rheum Dis. 2023. PMID: 33985940 No abstract available.
-
Response to: 'Correspondence on 'Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician reported registry'' by Rosenbaum et al.Ann Rheum Dis. 2023 Jun;82(6):e139. doi: 10.1136/annrheumdis-2021-220613. Epub 2021 May 13. Ann Rheum Dis. 2023. PMID: 33985941 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
