

Laboratory Diagnosis of Lyme Borreliosis
- PMID: 33504503
- PMCID: PMC7849240
- DOI: 10.1128/CMR.00018-19
Laboratory Diagnosis of Lyme Borreliosis
Abstract
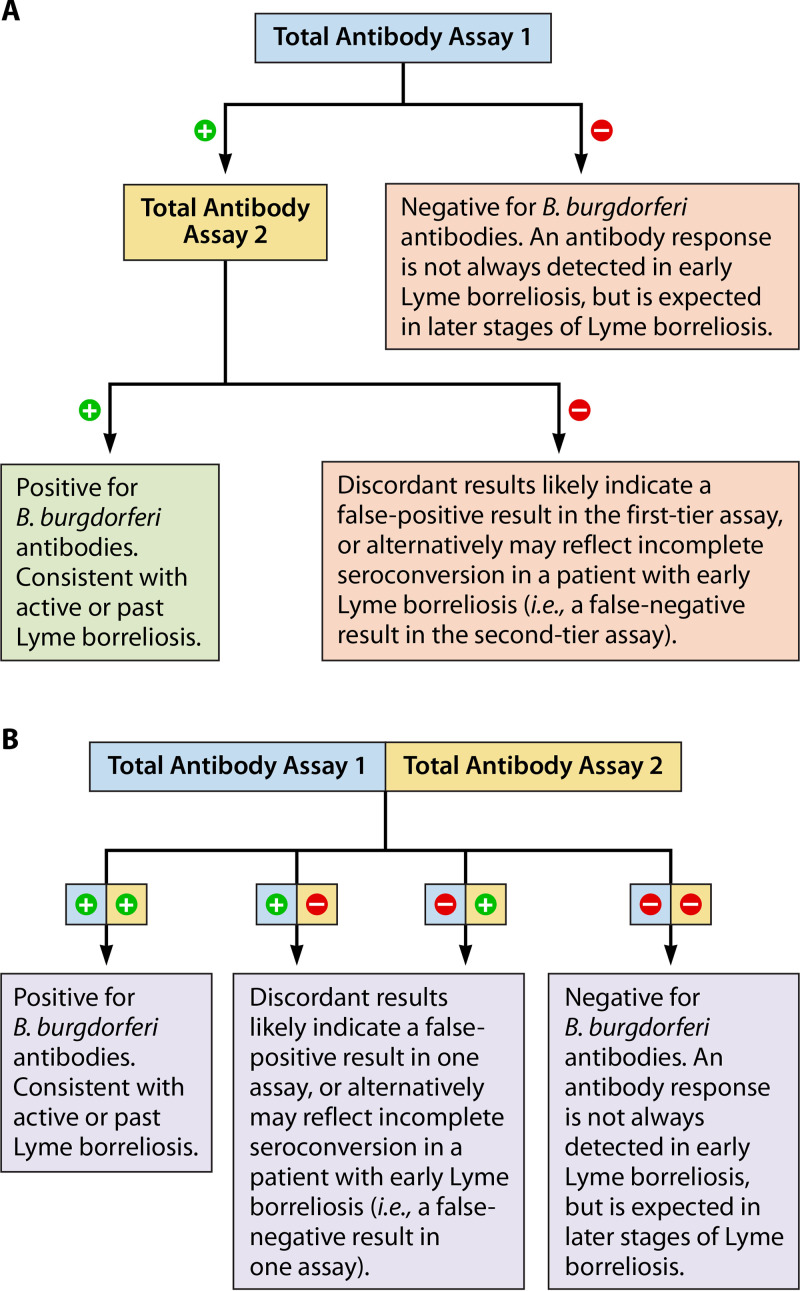
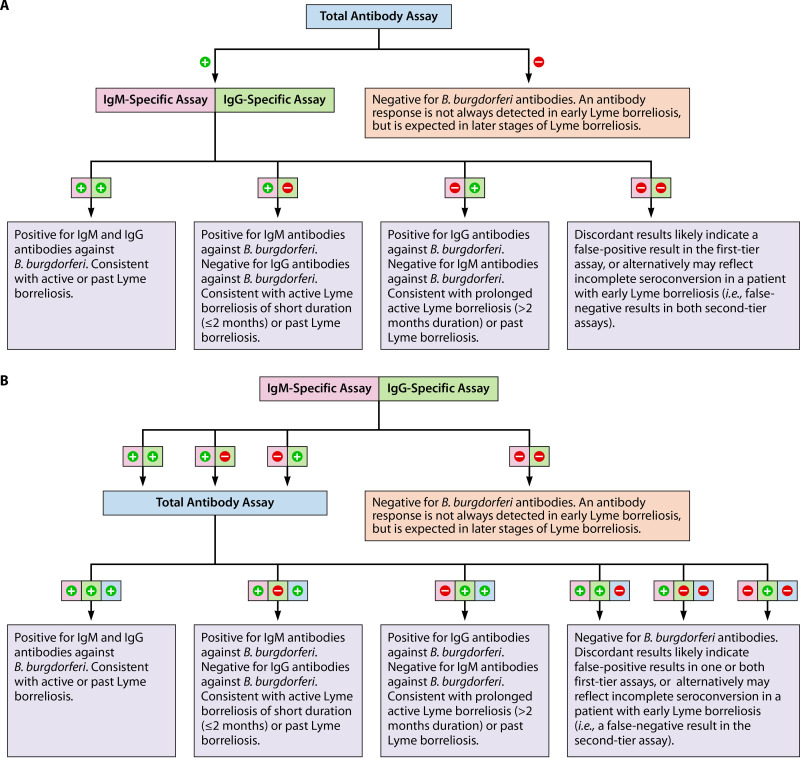
Lyme borreliosis is caused by a growing list of related, yet distinct, spirochetes with complex biology and sophisticated immune evasion mechanisms. It may result in a range of clinical manifestations involving different organ systems, and can lead to persistent sequelae in a subset of cases. The pathogenesis of Lyme borreliosis is incompletely understood, and laboratory diagnosis, the focus of this review, requires considerable understanding to interpret the results correctly. Direct detection of the infectious agent is usually not possible or practical, necessitating a continued reliance on serologic testing. Still, some important advances have been made in the area of diagnostics, and there are many promising ideas for future assay development. This review summarizes the state of the art in laboratory diagnostics for Lyme borreliosis, provides guidance in test selection and interpretation, and highlights future directions.
Keywords: Borrelia; Borrelia burgdorferi; Borreliella; Lyme disease; borreliosis; diagnosis; diagnostics; molecular methods; serology.
Copyright © 2021 American Society for Microbiology.
Figures

References
-
- Adeolu M, Gupta RS. 2014. A phylogenomic and molecular marker based proposal for the division of the genus Borrelia into two genera: the emended genus Borrelia containing only the members of the relapsing fever Borrelia, and the genus Borreliella gen. nov. containing the members of the Lyme disease Borrelia (Borrelia burgdorferi sensu lato complex. Antonie Van Leeuwenhoek 105:1049–1072. doi: 10.1007/s10482-014-0164-x. - DOI - PubMed
-
- Margos G, Castillo-Ramirez S, Cutler S, Dessau RB, Eikeland R, Estrada-Pena A, Gofton A, Grana-Miraglia L, Hunfeld KP, Krause A, Lienhard R, Lindgren PE, Oskam C, Rudolf I, Schwartz I, Sing A, Stevenson B, Wormser GP, Fingerle V. 2020. Rejection of the name Borreliella and all proposed species comb. nov. placed therein. Int J Syst Evol Microbiol 70:3577–3581. doi: 10.1099/ijsem.0.004149. - DOI - PubMed
-
- Stevenson B, Fingerle V, Wormser GP, Margos G. 2019. Public health and patient safety concerns merit retention of Lyme borreliosis-associated spirochetes within the genus Borrelia, and rejection of the genus novum Borreliella. Ticks Tick Borne Dis 10:1–4. doi: 10.1016/j.ttbdis.2018.08.010. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
