

Engineering biopharmaceutical formulations to improve diabetes management
- PMID: 33504649
- PMCID: PMC8004356
- DOI: 10.1126/scitranslmed.abd6726
Engineering biopharmaceutical formulations to improve diabetes management
Abstract
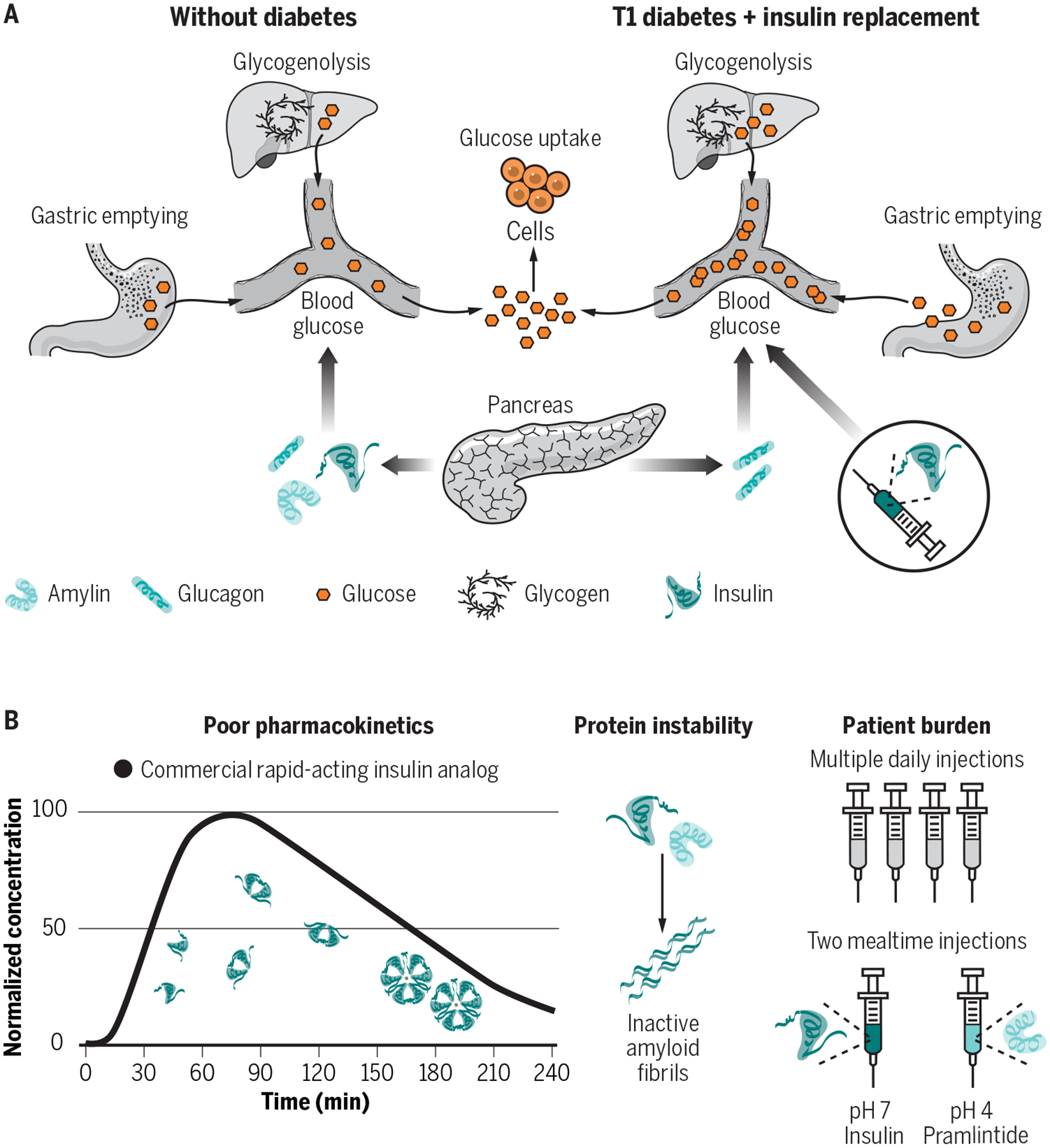
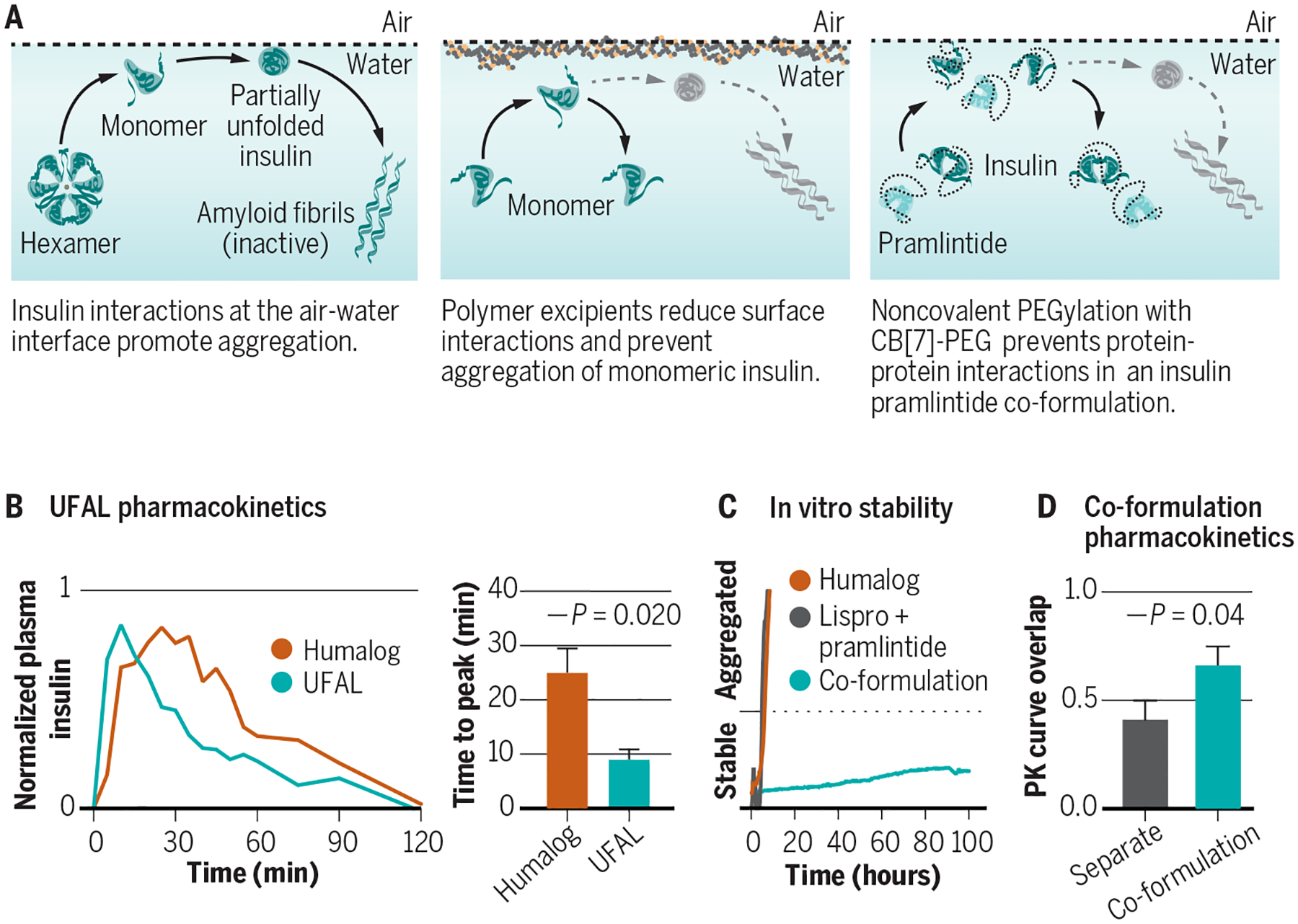
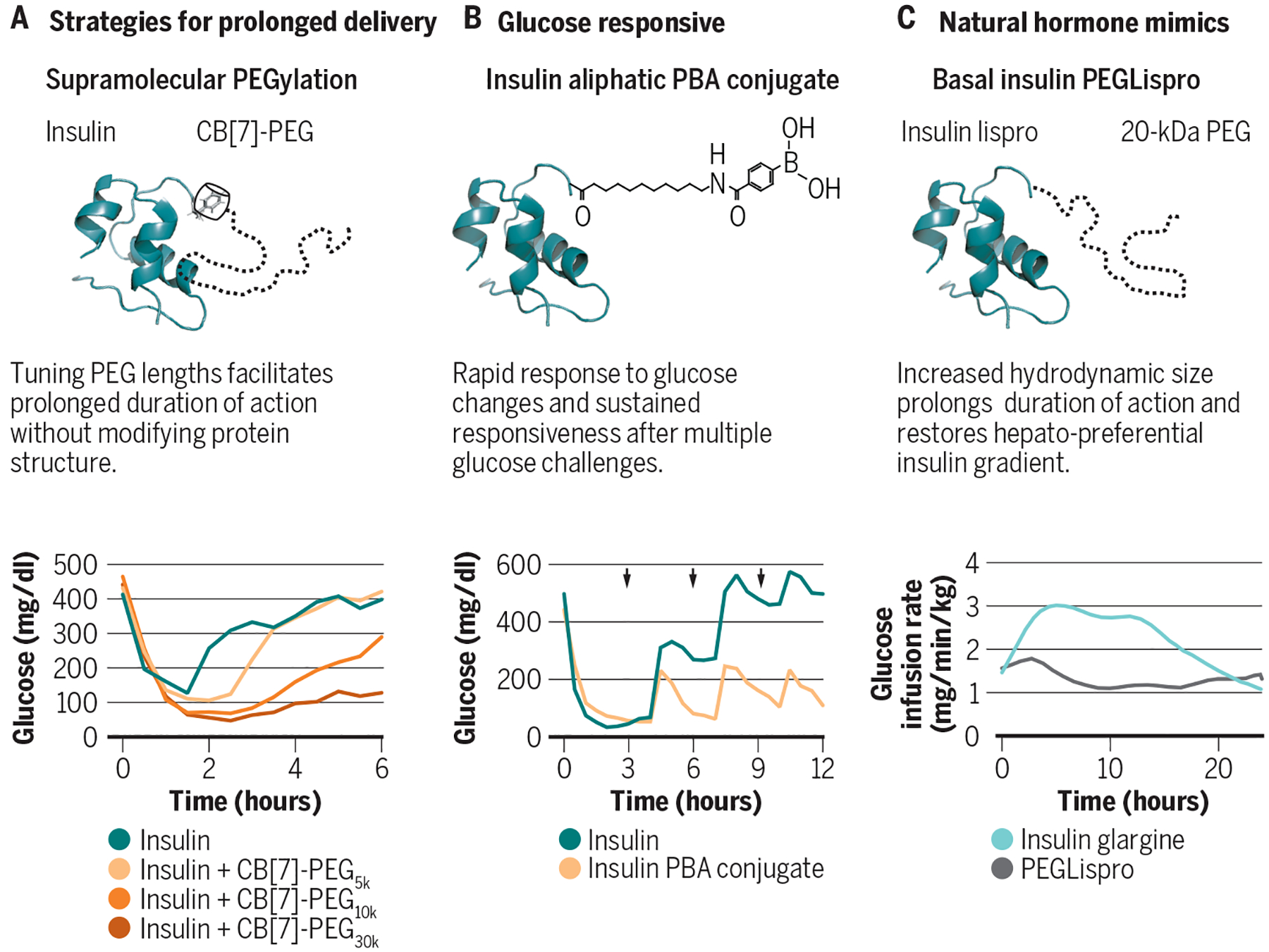
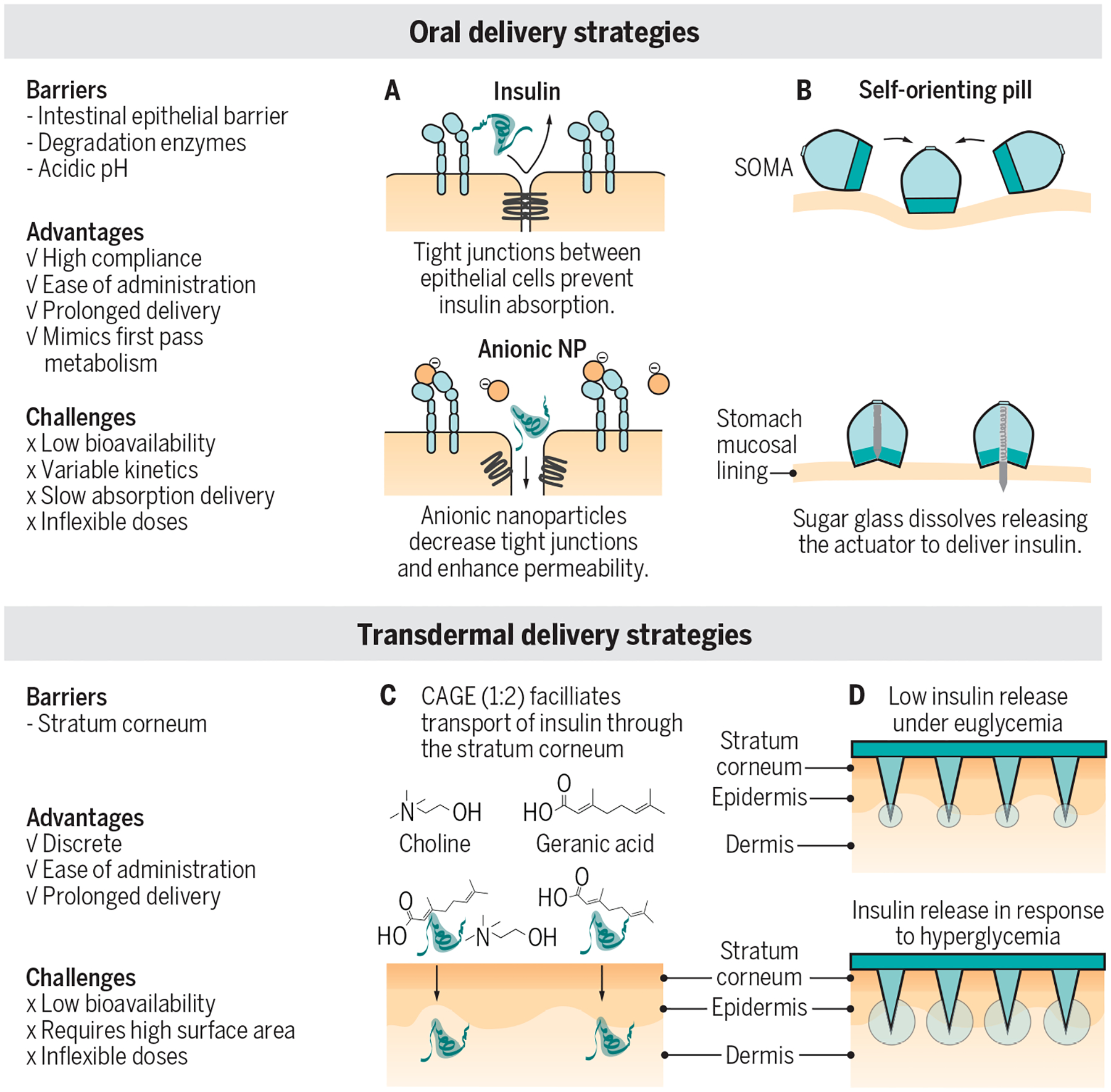
Insulin was first isolated almost a century ago, yet commercial formulations of insulin and its analogs for hormone replacement therapy still fall short of appropriately mimicking endogenous glycemic control. Moreover, the controlled delivery of complementary hormones (such as amylin or glucagon) is complicated by instability of the pharmacologic agents and complexity of maintaining multiple infusions. In this review, we highlight the advantages and limitations of recent advances in drug formulation that improve protein stability and pharmacokinetics, prolong drug delivery, or enable alternative dosage forms for the management of diabetes. With controlled delivery, these formulations could improve closed-loop glycemic control.
Copyright © 2021 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
COMPETING INTERESTS
E.A.A. and C.L.M. are inventors on provisional patent applications 63/011,928 and 62/948,159 filed by Stanford University describing some of the technology reported in this review. E.A.A., B.A.B, and C.L.M are inventors on a provisional patent application 62/804,357 filed by Stanford University describing some of the technology reported in this manuscript.
Figures
References
-
- Heptulla RA, Rodriguez LM, Bomgaars L, Haymond MW, The Role of Amylin and Glucagon in the Dampening of Glycemic Excursions in Children With Type 1 Diabetes. Diabetes 54, 1100 (2005). - PubMed
-
- Martin C, The Physiology of Amylin and Insulin: Maintaining the Balance Between Glucose Secretion and Glucose Uptake. Diabetes Educ 32, 101S–104S (2006). - PubMed
-
- Lebovitz HE, Adjunct therapy for type 1 diabetes mellitus. Nature Reviews Endocrinology 6, 326–334 (2010). - PubMed
-
- Aronoff SL, Berkowitz K, Shreiner B, Want L, Glucose Metabolism and Regulation: Beyond Insulin and Glucagon. Diabetes Spectrum 17, 183 (2004).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
