

Detection of colorectal cancer in urine using DNA methylation analysis
- PMID: 33504902
- PMCID: PMC7840909
- DOI: 10.1038/s41598-021-81900-6
Detection of colorectal cancer in urine using DNA methylation analysis
Abstract
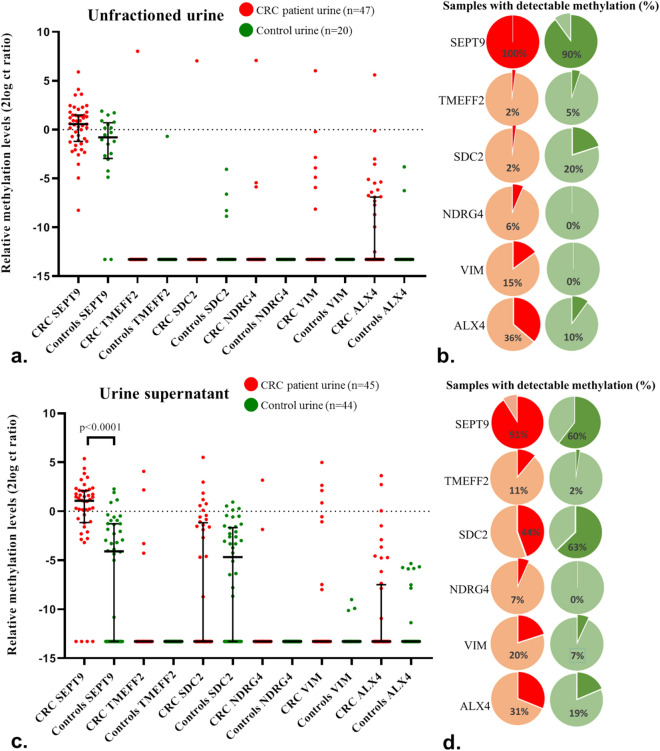
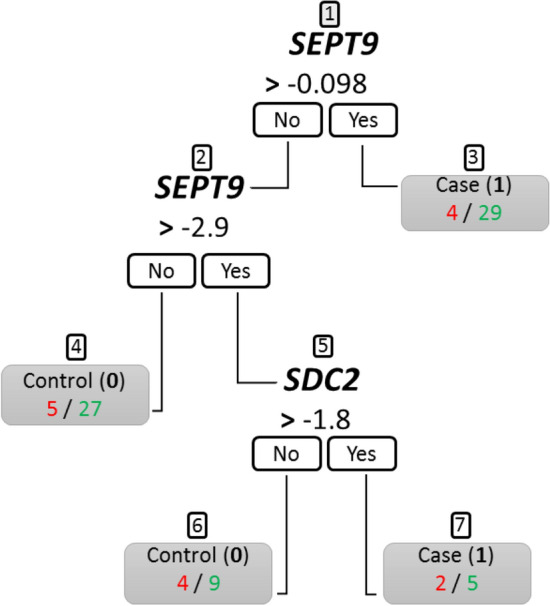
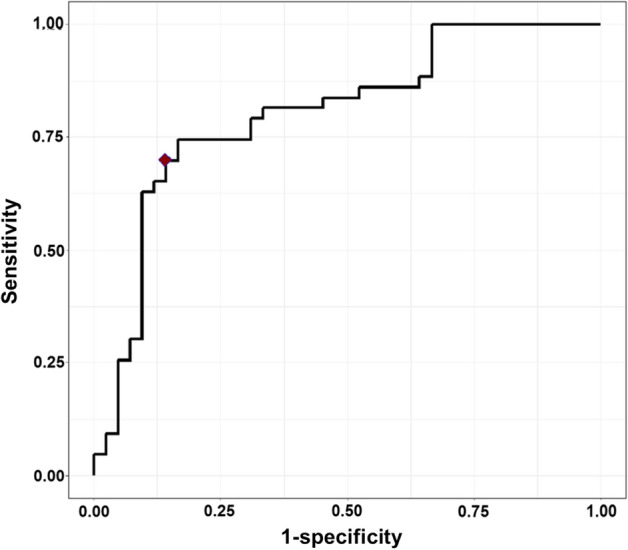
Colorectal cancer (CRC) is the second leading cause for cancer-related death globally. Clinically, there is an urgent need for non-invasive CRC detection. This study assessed the feasibility of CRC detection by analysis of tumor-derived methylated DNA fragments in urine. Urine samples, including both unfractioned and supernatant urine fractions, of 92 CRC patients and 63 healthy volunteers were analyzed for DNA methylation levels of 6 CRC-associated markers (SEPT9, TMEFF2, SDC2, NDRG4, VIM and ALX4). Optimal marker panels were determined by two statistical approaches. Methylation levels of SEPT9 were significantly increased in urine supernatant of CRC patients compared to controls (p < 0.0001). Methylation analysis in unfractioned urine appeared inaccurate. Following multivariate logistic regression and classification and regression tree analysis, a marker panel consisting of SEPT9 and SDC2 was able to detect up to 70% of CRC cases in urine supernatant at 86% specificity. First evidence is provided for CRC detection in urine by SEPT9 methylation analysis, which combined with SDC2 allows for an optimal differentiation between CRC patients and controls. Urine therefore provides a promising liquid biopsy for non-invasive CRC detection.
Conflict of interest statement
R.D.M.S has a minority stake in Self-screen B.V., a spin-off company of VU University Medical Center Amsterdam. R.D.M.S., S.B., I.B. and G.K. are named inventors on patent application(s) related to the detection of cancer DNA in urine. All other authors have no conflict of interest to declare.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
