

Low-Dose Methoxyflurane versus Standard of Care Analgesics for Emergency Trauma Pain: A Systematic Review and Meta-Analysis of Pooled Data
- PMID: 33505170
- PMCID: PMC7829133
- DOI: 10.2147/JPR.S292521
Low-Dose Methoxyflurane versus Standard of Care Analgesics for Emergency Trauma Pain: A Systematic Review and Meta-Analysis of Pooled Data
Abstract
Purpose: Undertreatment of trauma-related pain is common in the pre-hospital and hospital settings owing to barriers to the use of traditional standard of care analgesics. Low-dose methoxyflurane is an inhaled non-opioid analgesic with a rapid onset of pain relief that is approved for emergency relief of moderate-to-severe trauma-related pain in adults. This analysis was performed to compare the efficacy and safety of low-dose methoxyflurane with standard of care analgesics in adults with trauma-related pain.
Methods: A meta-analysis was performed on pooled data from randomized controlled trials identified via a systematic review. The primary endpoint was the pain intensity difference between baseline and various time intervals (5, 10, 15, 20, and 30 minutes) after initiation of treatment.
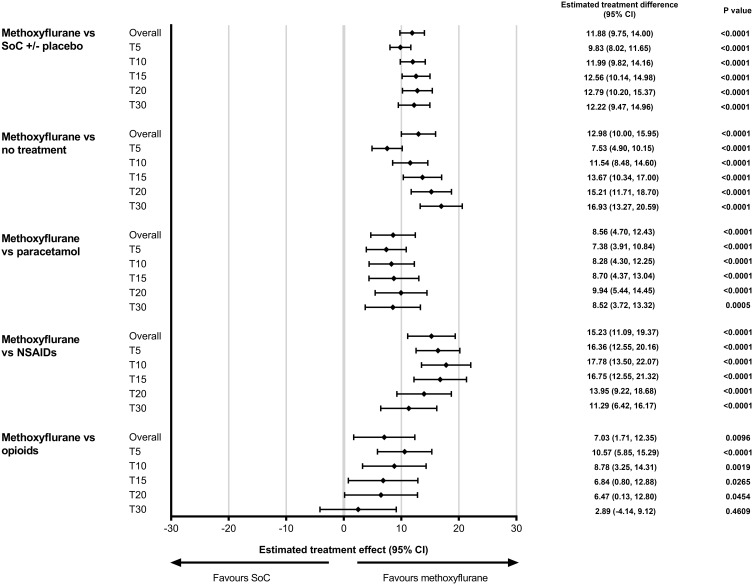
Results: The pain intensity difference was statistically superior with low-dose methoxyflurane compared with standard of care analgesics (overall estimated treatment effect=11.88, 95% CI=9.75-14.00; P<0.0001). The superiority of low-dose methoxyflurane was demonstrated at 5 minutes after treatment initiation and was maintained across all timepoints. Significantly more patients treated with methoxyflurane achieved response criteria of pain intensity ≤30 mm on a visual analog scale, and relative reductions in pain intensity of ≥30% and ≥50%, compared with patients who received standard of care analgesics. The median time to pain relief was shorter with methoxyflurane than with standard of care analgesics. The findings were consistent in a subgroup of elderly patients (aged ≥65 years).
Conclusion: Methoxyflurane can be considered as an alternative to standard of care analgesics in pre-hospital and hospital settings for treatment of adult patients with acute trauma-related pain.
Keywords: acute pain; analgesia; emergency service; inhaled analgesic; pain management; wounds and injury.
© 2021 Fabbri et al.
Conflict of interest statement
Dr Fabbri has received fees from Mundipharma as a member of the scientific committee for the MEDITA study, and was corresponding author for that study. Dr Borobia has received fees from Mundipharma as a member of the scientific committee for InMEDIATE, as well as speaker fees from Mundipharma and Menarini. Dr Borobia is Principal Investigator on clinical trials sponsored by GSK, Daiichi Sankyo, Janssen and Farmalider. Dr Ricard-Hibon has served as an advisory board member for Mundipharma. Professor Coffey was chief investigator for the STOP! Study and has received honoraria to present at symposia sponsored by Mundipharma. Aurore Caumont-Prim and François Montestruc are employees of eXYSTAT, a contract research organization which received fees from Mundibiopharma Limited to perform the meta-analysis. Amedeo Soldi is an employee of Mundipharma Srl. Susana Traseira Lugilde is an employee of Mundipharma S.L. Sara Dickerson is an employee of Mundibiopharma Limited. The authors report no other conflicts of interest in this work.
Figures


Similar articles
-
Clinical assessment and risk stratification for prehospital use of methoxyflurane versus standard analgesia in adult patients with trauma pain.Turk J Emerg Med. 2023 Jan 27;23(2):65-74. doi: 10.4103/tjem.tjem_229_22. eCollection 2023 Apr-Jun. Turk J Emerg Med. 2023. PMID: 37169029 Free PMC article. Review.
-
Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane Versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA).Adv Ther. 2019 Nov;36(11):3030-3046. doi: 10.1007/s12325-019-01055-9. Epub 2019 Oct 12. Adv Ther. 2019. PMID: 31612359 Free PMC article. Clinical Trial.
-
Inhaled Methoxyflurane Provides Greater Analgesia and Faster Onset of Action Versus Standard Analgesia in Patients With Trauma Pain: InMEDIATE: A Randomized Controlled Trial in Emergency Departments.Ann Emerg Med. 2020 Mar;75(3):315-328. doi: 10.1016/j.annemergmed.2019.07.028. Epub 2019 Oct 14. Ann Emerg Med. 2020. PMID: 31623936 Clinical Trial.
-
Inhaled Methoxyflurane versus Intravenous Morphine for Severe Trauma Pain in the Emergency Setting: Subgroup Analysis of MEDITA, a Multicenter, Randomized, Controlled, Open-Label Trial.J Pain Res. 2020 Mar 6;13:491-502. doi: 10.2147/JPR.S240911. eCollection 2020. J Pain Res. 2020. PMID: 32184653 Free PMC article.
-
[Volatile anesthetics for prehospital analgesia by paramedics-An overview].Anaesthesist. 2022 Mar;71(3):233-242. doi: 10.1007/s00101-021-01051-1. Epub 2021 Oct 18. Anaesthesist. 2022. PMID: 34664081 Free PMC article. Review. German.
Cited by
-
Parenteral, Non-Intravenous Analgesia in Acute Traumatic Pain-A Narrative Review Based on a Systematic Literature Search.J Clin Med. 2024 Apr 26;13(9):2560. doi: 10.3390/jcm13092560. J Clin Med. 2024. PMID: 38731088 Free PMC article. Review.
-
The 2023 WSES guidelines on the management of trauma in elderly and frail patients.World J Emerg Surg. 2024 May 31;19(1):18. doi: 10.1186/s13017-024-00537-8. World J Emerg Surg. 2024. PMID: 38816766 Free PMC article.
-
Clinical assessment and risk stratification for prehospital use of methoxyflurane versus standard analgesia in adult patients with trauma pain.Turk J Emerg Med. 2023 Jan 27;23(2):65-74. doi: 10.4103/tjem.tjem_229_22. eCollection 2023 Apr-Jun. Turk J Emerg Med. 2023. PMID: 37169029 Free PMC article. Review.
-
The Pain Management of Trauma Patients in the Emergency Department.J Clin Med. 2023 May 5;12(9):3289. doi: 10.3390/jcm12093289. J Clin Med. 2023. PMID: 37176729 Free PMC article. Review.
References
-
- European Society for Emergency Medicine. Guidelines for the management of acute pain in emergency situations; 2020. Available from: https://www.eusem.org/images/EUSEM_EPI_GUIDELINES_MARCH_2020.pdf. Accessed September23, 2020.
LinkOut - more resources
Full Text Sources
Other Literature Sources
