

Novel Subgroups in Subarachnoid Hemorrhage and Their Association With Outcomes-A Systematic Review and Meta-Regression
- PMID: 33505300
- PMCID: PMC7829354
- DOI: 10.3389/fnagi.2020.573454
Novel Subgroups in Subarachnoid Hemorrhage and Their Association With Outcomes-A Systematic Review and Meta-Regression
Abstract
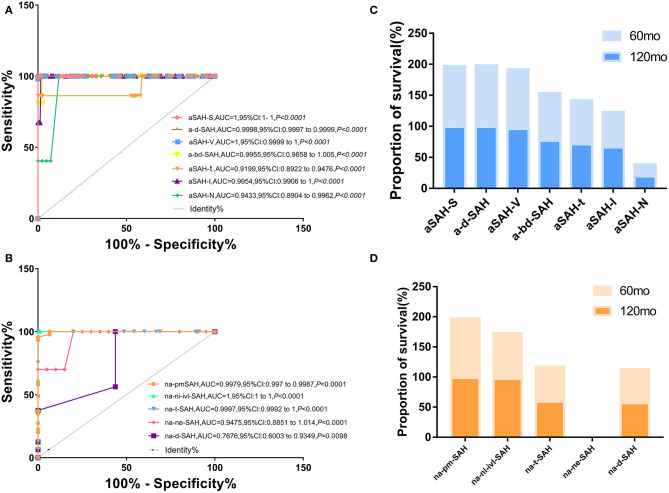
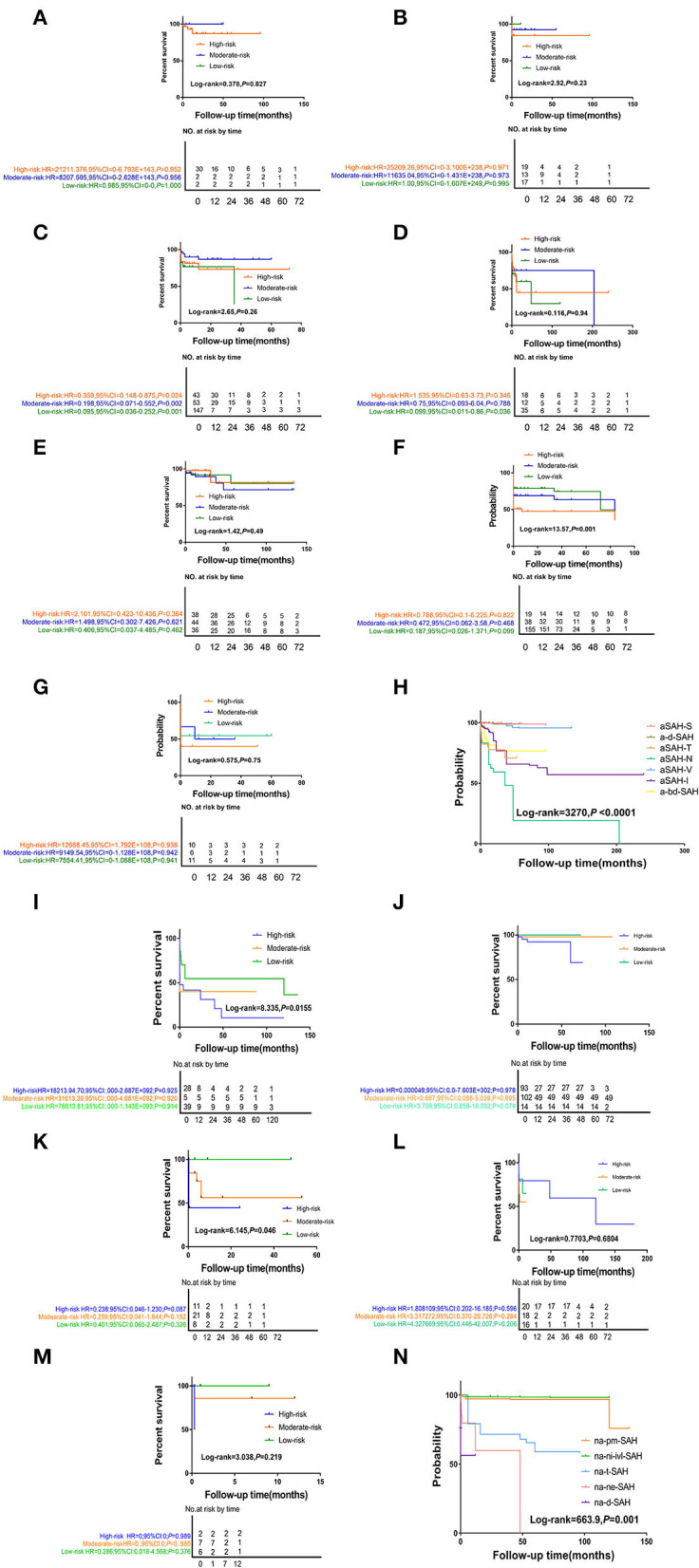
Background and Purpose: Subarachnoid hemorrhage (SAH) has long been classified into two main forms, aneurysmal SAH (aSAH) and non-aneurysmal SAH (naSAH), but the related risk factors for aSAH and naSAH are heterogeneous. Our objective was to determine the risk factors for SAH of known or unknown origin with respect to diagnostic evaluation in a large patient cohort. We sought to determine whether our classification system can further predict middle long-term stroke and death. Methods: We performed a systematic review and meta-analysis to identify risk factors for each SAH subtype. The discovery phase analyzed 11 risk factors from case studies in the literature. Kruskal-Wallis, Cox regression, logistic regression, and Kaplan-Meier analyses were used to compare the two groups. Results: A total of 14,904 (34.53%) male and 22,801 (52.84%) female patients were eligible for this study. At a median follow-up of 45.6 months, the 5-years overall survival was 97.768% (95% CI: 0.259-0.292) for aSAH patients and 87.904% (95% CI: 1.459-1.643) for naSAH patients. The 10-years survival rate was 93.870% (95% CI: 2.075-3.086) and 78.115% (95% CI: 2.810-3.156), respectively. Multi-risk factor subgroups showed significant intergroup differences. We identified eight risk factors (drugs, trauma, neoplastic, vessels lesion, inflammatory lesion, blood disease, aneurysm, peri-mesencephalic hemorrhage) using logistic regression, which were optimally differentiated among the aSAH [aSAH-S (AUC: 1), a-d-SAH (AUC: 0.9998), aSAH-T (AUC: 0.9199), aSAH-N (AUC: 0.9433), aSAH-V (AUC: 1), aSAH-I (AUC: 0.9954), a-bd-SAH (AUC: 0.9955)] and naSAH [na-pmSAH (AUC: 0.9979), na-ni-ivl-SAH (AUC: 1), na-t-SAH (AUC: 0.9997), na-ne-SAH (AUC: 0.9475), na-d-SAH (AUC: 0.7676)] subgroups. These models were applied in a parallel cohort, showing eight risk factors plus survival rates to predict the prognosis of SAH. Conclusions: The classification of risk factors related to aSAH and naSAH is helpful in the diagnosis and prediction of the prognosis of aSAH and naSAH patients. Further validation is needed in future clinical applications.
Keywords: cohort studies; follow up risk time points; related-risk factors disease; risk factors; subgroup subarachnoid hemorrhage.
Copyright © 2021 Wang, Fu, Song, Ma, Zhang and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Re-Evaluating Risk Factors, Incidence, and Outcome of Aneurysmal and Non-Aneurysmal Subarachnoid Hemorrhage.World Neurosurg. 2023 Jul;175:e492-e504. doi: 10.1016/j.wneu.2023.03.131. Epub 2023 Apr 5. World Neurosurg. 2023. PMID: 37024083
-
Demographic, circadian, and climatic factors in non-aneurysmal versus aneursymal subarachnoid hemorrhage.Clin Neurol Neurosurg. 2013 Mar;115(3):298-303. doi: 10.1016/j.clineuro.2012.05.039. Epub 2012 Jul 6. Clin Neurol Neurosurg. 2013. PMID: 22770541
-
Exploration of Risk Factors for Poor Prognosis of Non-Traumatic Non-Aneurysmal Subarachnoid Hemorrhage.Biomolecules. 2022 Jul 6;12(7):948. doi: 10.3390/biom12070948. Biomolecules. 2022. PMID: 35883504 Free PMC article.
-
Statins Improve Clinical Outcome After Non-aneurysmal Subarachnoid Hemorrhage: A Translational Insight From a Systematic Review of Experimental Studies.Front Neurol. 2021 May 14;12:620096. doi: 10.3389/fneur.2021.620096. eCollection 2021. Front Neurol. 2021. PMID: 34054685 Free PMC article.
-
Prognostic value of elevated cardiac troponin in aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis.Front Neurol. 2025 Mar 18;16:1506819. doi: 10.3389/fneur.2025.1506819. eCollection 2025. Front Neurol. 2025. PMID: 40170897 Free PMC article.
Cited by
-
Current status of perimesencephalic non-aneurysmal subarachnoid hemorrhage.Front Neurol. 2022 Sep 1;13:960702. doi: 10.3389/fneur.2022.960702. eCollection 2022. Front Neurol. 2022. PMID: 36119687 Free PMC article. Review.
-
Systemic Inflammatory Response in Spontaneous Subarachnoid Hemorrhage from Aneurysmal Rupture versus Subarachnoid Hemorrhage of Unknown Origin.J Inflamm Res. 2022 Nov 16;15:6329-6342. doi: 10.2147/JIR.S380101. eCollection 2022. J Inflamm Res. 2022. PMID: 36415221 Free PMC article.
-
Clinical outcome and prognostic factors of patients with non-traumatic angiography-negative subarachnoid hemorrhage.Front Neurol. 2023 Jul 20;14:1157845. doi: 10.3389/fneur.2023.1157845. eCollection 2023. Front Neurol. 2023. PMID: 37545726 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources