

Case Reports
doi: 10.1155/2021/8862405.
eCollection 2021.
Scleroderma Renal Crisis in a Case of Mixed Connective Tissue Disease Treated Successfully with Angiotensin-Converting Enzyme Inhibitors
Affiliations
- PMID: 33505743
- PMCID: PMC7808802
- DOI: 10.1155/2021/8862405
Item in Clipboard
Case Reports
Scleroderma Renal Crisis in a Case of Mixed Connective Tissue Disease Treated Successfully with Angiotensin-Converting Enzyme Inhibitors
Case Rep Nephrol.
.
Abstract
Mixed connective tissue disease (MCTD) is a rheumatic disease syndrome with overlapping features of scleroderma, systemic lupus erythematosus, and polymyositis. An extremely rare but serious complication that can occur in MCTD is scleroderma renal crisis (SRC). There have been different approaches to the treatment of SRC associated with MCTD. We present a case of MCTD with chronic features of Raynaud's phenomenon, dermatomyositis, and thrombocytopenia complicated with acute SRC which showed a great response to ACE inhibitors. Here, we advise the early and aggressive use of ACE inhibitors as soon as SRC is suspected.
Copyright © 2021 Jomana Madieh et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
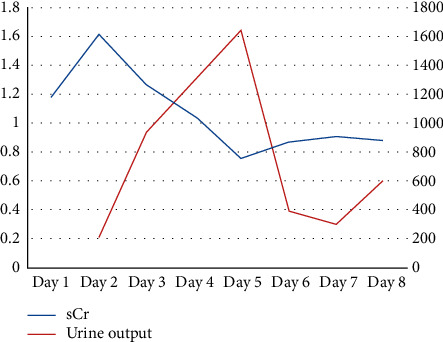
Serum creatinine trend (blue line) and urine output trend (red line) throughout patient's hospitalization.
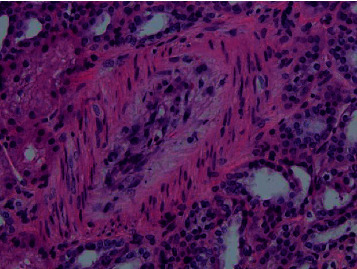
Edematous mucoid intimal thickening of interlobular artery (H&E).
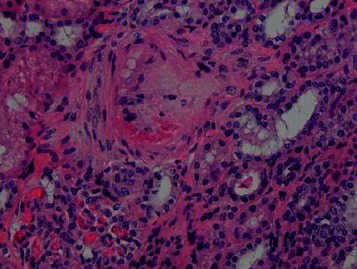
Intimal fibrinoid changes in interlobular artery (H&E).

Intimal fibrinoid changes in interlobular artery (trichrome stain). Same interlobular artery is shown in figure 3.

Normal glomeruli (PAS).
Similar articles
-
Scleroderma renal crisis in a newly diagnosed mixed connective tissue disease resulting in dialysis-dependent chronic kidney disease despite angiotensin-converting enzyme inhibition.CEN Case Rep. 2013 May;2(1):41-45. doi: 10.1007/s13730-012-0036-z. Epub 2012 Sep 28. CEN Case Rep. 2013. PMID: 28509217 Free PMC article.
-
Scleroderma renal crisis in a case of mixed connective tissue disease.Saudi J Kidney Dis Transpl. 2014 Jul;25(4):844-8. doi: 10.4103/1319-2442.135177. Saudi J Kidney Dis Transpl. 2014. PMID: 24969199 Review.
-
The dilemma: scleroderma renal crisis vs lupus nephritis in a patient with mixed connective tissue disorder.J Community Hosp Intern Med Perspect. 2021 Nov 15;11(6):852-855. doi: 10.1080/20009666.2021.1983320. eCollection 2021. J Community Hosp Intern Med Perspect. 2021. PMID: 34804405 Free PMC article.
-
Scleroderma Renal Crisis in Mixed Connective Tissue Disease With Full Renal Recovery Within 3 Months: A Case Report With Expanding Treatment Modalities to Treat Each Clinical Sign as an Independent Entity.J Investig Med High Impact Case Rep. 2017 Oct 10;5(4):2324709617734012. doi: 10.1177/2324709617734012. eCollection 2017 Oct-Dec. J Investig Med High Impact Case Rep. 2017. PMID: 29051891 Free PMC article.
-
Mixed connective tissue disease.Lupus. 2006;15(3):132-7. doi: 10.1191/0961203306lu2283rr. Lupus. 2006. PMID: 16634365 Review.
Cited by
-
Challenging diagnosis of renal failure associated with severe neurological symptoms in a patient with mixed connective tissue disease.J Scleroderma Relat Disord. 2023 Feb;8(1):NP6-NP10. doi: 10.1177/23971983221099847. Epub 2022 Jun 13. J Scleroderma Relat Disord. 2023. PMID: 36743813 Free PMC article.
References
-
- Sharp G. C., Irvin W. S., Tan E. M., Gould R. G., Holman H. R. Mixed connective tissue disease-an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA) The American Journal of Medicine. 1972;52(2):148–159. doi: 10.1016/0002-9343(72)90064-2. - DOI - PubMed
-
- Cheta J., Rijhwani S., Rust H. Scleroderma renal crisis in mixed connective tissue disease with full renal recovery within 3 months: a case report with expanding treatment modalities to treat each clinical sign as an independent entity. Journal of Investigative Medicine High Impact Case Report. 2017;5(4):1–5. doi: 10.1177/2324709617734012. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
