

Case Reports
doi: 10.1016/j.hrcr.2020.10.009.
eCollection 2021 Jan.
How to map and ablate a pulmonary vein-to-right atrium breakthrough during simultaneous persistent pulmonary vein fibrillation and organized atrial fibrillation using an automated high-resolution mapping system
Affiliations
- PMID: 33505854
- PMCID: PMC7813795
- DOI: 10.1016/j.hrcr.2020.10.009
Item in Clipboard
Case Reports
How to map and ablate a pulmonary vein-to-right atrium breakthrough during simultaneous persistent pulmonary vein fibrillation and organized atrial fibrillation using an automated high-resolution mapping system
HeartRhythm Case Rep.
.
No abstract available
Keywords: Atrial fibrillation; Epicardial conduction; High-resolution mapping; Intercaval bundle fiber; Pulmonary vein reconnection.
Figures

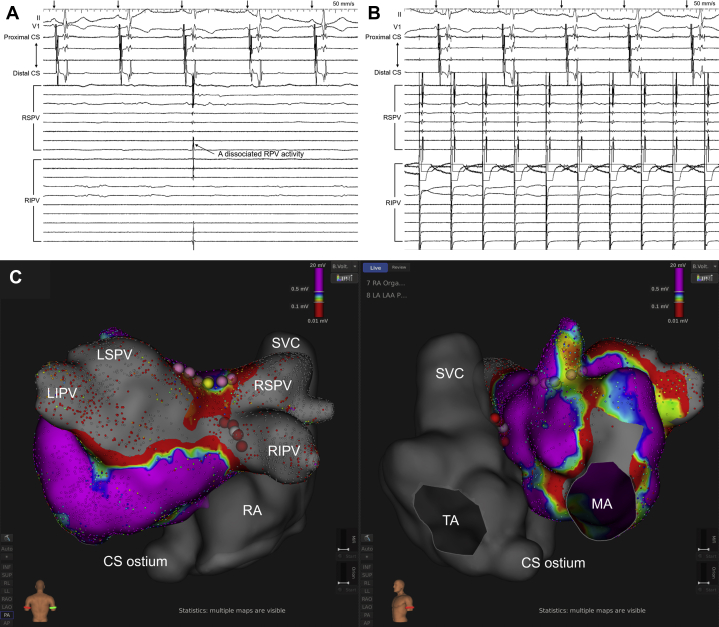
A: Body surface and intracardiac electrograms during the atrial fibrillation (AF). The right pulmonary vein (PV) electrograms revealed disorganized activation and a shorter cycle length (CL) compared to the atrial electrograms recorded within the coronary sinus (CS), while the CS electrograms did not always reveal a stable CL and consistent activation sequence but revealed relatively organized activation. The numbers indicate the CLs measured in the CS. B: Automated atrial electrogram acquisition during the AF. During activation mapping, the beats that met all beat acceptance criteria were automatically acquired (green arrowheads), but those that did not meet any of the criteria were excluded (red arrowheads). The upper panels show whether each criterion was met or not: CL, CL variation (±70 ms); ΔR, activation timing difference between 2 reference electrodes (±5 ms); RSP, respiration gating; M, catheter motion per beat (<1 mm); S, catheter electrogram stability (0.25); TR, catheter tracking quality (<3). In the present case, the CL variation was manually set at ±70 ms, but the other parameters were the default values of the system. The bar became green if each criterion was met, and in contrast the bar became red if not. The middle panel shows the intracardiac electrograms recorded by the multielectrode catheter in the CS and the mini-basket catheter in the atrium. The numbers indicate the CLs measured by the reference electrode in the CS (CS 3-4). The lower panel shows the real-time curve of the CL, which fluctuated intensely between 210 and 430 ms. The green area in the lower panel indicates the acceptance threshold of the CL, and the upper and lower acceptance thresholds are 452 ms and 312 ms, respectively. If the CL was within the green area, the beat met the criterion of the CL variation, but if the CL was outside the green area, the beat did not. A4-5 to H4-5, mini-basket catheter recordings. CS1-2 to CS8-9, distal to proximal coronary sinus recordings. RIPV = right inferior PV electrograms recorded by a circular mapping catheter; RSPV = right superior PV electrograms recorded by the mini-basket catheter.

Activation maps in the atria during the organized AF exhibited (A, B) a centrifugal pattern with the earliest activation on the right atrial septum and (C, D) conduction to the left atrium (LA) via the atrial septum (Online Video). The left and right panels show the LA and right atrium (RA) in the left anterior oblique view and the RA only in the left posterior oblique view, respectively. The gray tags are placed along the previous pulmonary vein isolation lines, and the white, light green, and light blue tags represent the earliest activation site (EAS) in the RA, LA site on the opposite side of the EAS in the RA, and EAS in the LA, respectively. The dark red and white arrows on the maps represent the activation wavefront and activation propagation, respectively. The numbers in the local electrograms indicate the intervals from the reference electrogram recorded in the coronary sinus (CS) to the local electrogram. The projection distance and confidence mask for the maps and online video were set at 2 mm and 0.03 mV, respectively. IVC = inferior vena cava; LAA = left atrial appendage; LSPV = left superior pulmonary vein; MA = mitral annulus; RSPV = right superior pulmonary vein; SVC = superior vena cave; TA = tricuspid annulus.
A, B: Entrance block from the atria to the right pulmonary veins (RPVs) (A) and exit block from the RPVs to the atria (B) were verified during sinus rhythm and RPV pacing. The black arrows on the electrocardiograms indicate the P waves during sinus rhythm. C: Final radiofrequency (RF) ablation sites with the postablation left atrial voltage map in the posteroanterior (left panel) and left anterior oblique (right panel) views. The yellow and pink tags represent the conduction gap and RF ablation sites along the superior box isolation line, respectively. The white and red tags represent the earliest activation site during the organized atrial fibrillation and RF ablation sites on the right atrial septum, respectively. RPV = right pulmonary vein. The other abbreviations are as in Figures 1 and 2.
Similar articles
-
Epicardial Breakthrough Waves During Sinus Rhythm: Depiction of the Arrhythmogenic Substrate?Circ Arrhythm Electrophysiol. 2017 Sep;10(9):e005145. doi: 10.1161/CIRCEP.117.005145. Circ Arrhythm Electrophysiol. 2017. PMID: 28912205
-
Impact of Ischemic and Valvular Heart Disease on Atrial Excitation:A High-Resolution Epicardial Mapping Study.J Am Heart Assoc. 2018 Mar 8;7(6):e008331. doi: 10.1161/JAHA.117.008331. J Am Heart Assoc. 2018. PMID: 29519812 Free PMC article.
-
Epicardial connection between the right-sided pulmonary venous carina and the right atrium in patients with atrial fibrillation: A possible mechanism for preclusion of pulmonary vein isolation without carina ablation.Heart Rhythm. 2019 May;16(5):671-678. doi: 10.1016/j.hrthm.2018.11.017. Epub 2018 Nov 20. Heart Rhythm. 2019. PMID: 30465905
-
Role of endo-epicardial dissociation of electrical activity and transmural conduction in the development of persistent atrial fibrillation.Prog Biophys Mol Biol. 2014 Aug;115(2-3):173-85. doi: 10.1016/j.pbiomolbio.2014.07.007. Epub 2014 Jul 30. Prog Biophys Mol Biol. 2014. PMID: 25086270 Review.
-
Bi-atrial mapping of atrial arrhythmias.Card Electrophysiol Rev. 2002 Dec;6(4):378-82. doi: 10.1023/a:1021176123007. Card Electrophysiol Rev. 2002. PMID: 12438816 Review.
References
-
- Barrio-Lopez M.T., Sanchez-Quintana D., Garcia-Martinez J. Epicardial connections involving pulmonary veins: the prevalence, predictors, and implications for ablation outcome. Circ Arrhythm Electrophysiol. 2020;13 - PubMed
-
- Patel P.J., D'Souza B., Saha P., Chik W.W., Riley M.P., Garcia F.C. Electroanatomic mapping of the intercaval bundle in atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:1262–1267. - PubMed
-
- Yoshida K., Baba M., Shinoda Y. Epicardial connection between the right-sided pulmonary venous carina and the right atrium in patients with atrial fibrillation: A possible mechanism for preclusion of pulmonary vein isolation without carina ablation. Heart Rhythm. 2019;16:671–678. - PubMed
-
- Perez-Castellano N., Villacastin J., Salinas J. Epicardial connections between the pulmonary veins and left atrium: relevance for atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2011;22:149–159. - PubMed
-
- Anter E., McElderry T.H., Contreras-Valdes F.M. Evaluation of a novel high-resolution mapping technology for ablation of recurrent scar-related atrial tachycardias. Heart Rhythm. 2016;13:2048–2055. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
