

Predictors of CT Morphologic Features to Identify Spread Through Air Spaces Preoperatively in Small-Sized Lung Adenocarcinoma
- PMID: 33505903
- PMCID: PMC7831277
- DOI: 10.3389/fonc.2020.548430
Predictors of CT Morphologic Features to Identify Spread Through Air Spaces Preoperatively in Small-Sized Lung Adenocarcinoma
Abstract
Objectives: This study aimed to explore the predictive CT features of spread through air spaces (STAS) in patients with small-sized lung adenocarcinoma.
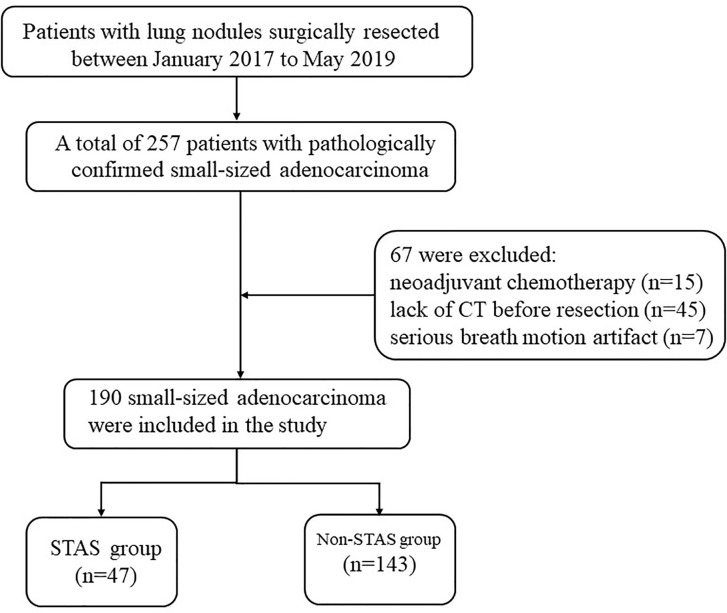
Methods: From January 2017 to May 2019, patients with confirmed pathology of small-sized lung adenocarcinoma (less than or equal to 2 cm) and who underwent surgery were retrospectively analyzed. The clinical, pathological, and surgical information and CT features were analyzed.
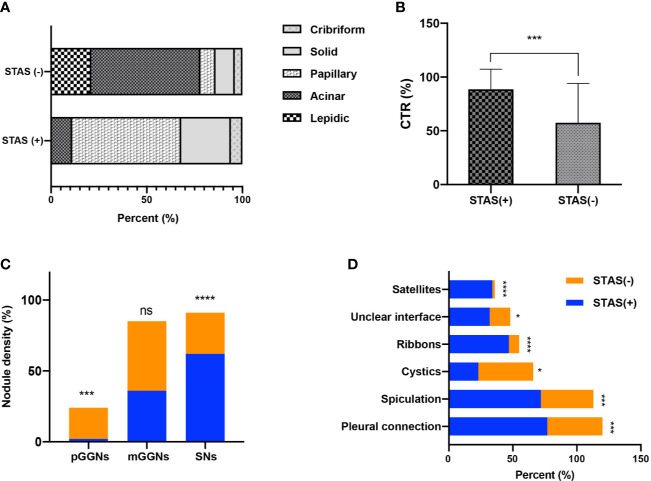
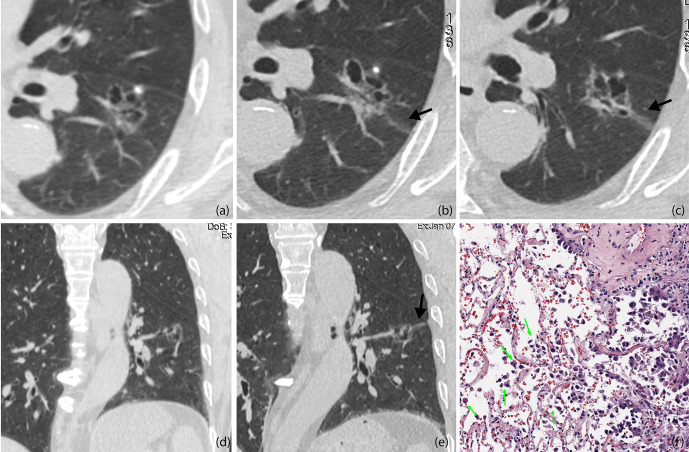
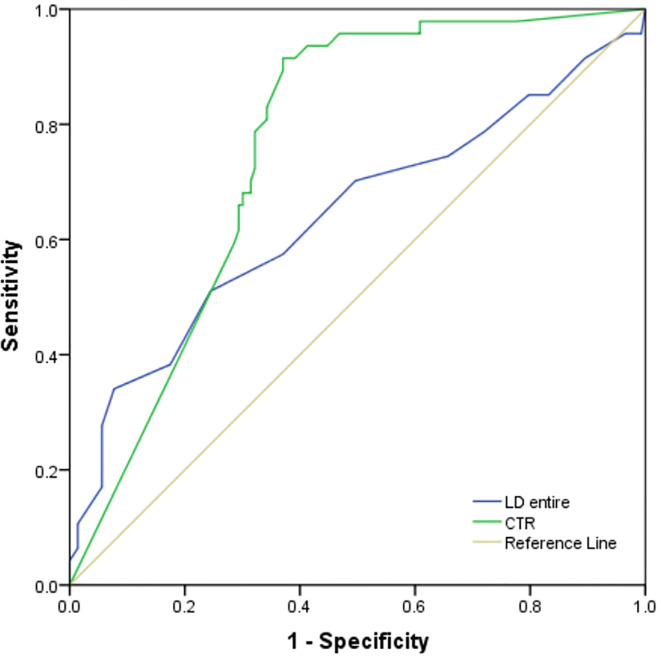
Results: A total of 47 patients with STAS (males, 61.7%; mean age, 56 ± 8years) and 143 patients without STAS (males, 58%; mean age, 53 ± 11 years) were included. Pathologically, papillary, micropapillary, solid predominant subtypes, and vascular and pleural invasion were most commonly observed features in the STAS group. Radiologically, higher consolidation tumor ratio (CTR), presence of spiculation, satellites, ground glass ribbon sign, pleural attachment, and unclear tumor-lung interface were more commonly observed features in the STAS group. CTR, presence of ground glass ribbons and pleural connection, and absence of cystic airspaces were considered as stable predictors of STAS in multivariate logistic models. The receiver operating characteristic curve (ROC) analysis for predicting STAS demonstrated higher area under the curve (AUC) in the model that used CTR (0.760, 95% confidence interval, 0.69-0.83) for predicting STAS than in the model that used long diameter of entire lesion (0.640).
Conclusions: CTR is the best CT sign for predicting STAS in small-sized lung adenocarcinoma. The ground glass ribbon is a newly found indicator and has the potential for predicting STAS.
Keywords: adenocarcinoma of lung; bronchial neoplasms; spread through air spaces; tomography; x-ray computed.
Copyright © 2021 Qi, Xue, Cai, Lu, Li and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Does dual-layer spectral detector CT provide added value in predicting spread through air spaces in lung adenocarcinoma? A preliminary study.Eur Radiol. 2024 Jun;34(6):4176-4186. doi: 10.1007/s00330-023-10440-6. Epub 2023 Nov 17. Eur Radiol. 2024. PMID: 37973632
-
Clinicopathological and CT features of tumor spread through air space in invasive lung adenocarcinoma.Front Oncol. 2022 Sep 23;12:959113. doi: 10.3389/fonc.2022.959113. eCollection 2022. Front Oncol. 2022. PMID: 36212429 Free PMC article.
-
The correlation between tumor radiological features and spread through air spaces in peripheral stage IA lung adenocarcinoma: a propensity score-matched analysis.J Cardiothorac Surg. 2024 Jan 23;19(1):19. doi: 10.1186/s13019-024-02498-0. J Cardiothorac Surg. 2024. PMID: 38263158 Free PMC article.
-
Computed Tomography Features and Tumor Spread Through Air Spaces in Lung Adenocarcinoma: A Meta-analysis.J Thorac Imaging. 2023 Mar 1;38(2):W19-W29. doi: 10.1097/RTI.0000000000000693. Epub 2022 Dec 28. J Thorac Imaging. 2023. PMID: 36583661 Free PMC article.
-
[Research Progress on Spread Through Air Spaces of Lung Cancer].Zhongguo Fei Ai Za Zhi. 2022 Jan 20;25(1):54-60. doi: 10.3779/j.issn.1009-3419.2021.101.49. Epub 2021 Dec 23. Zhongguo Fei Ai Za Zhi. 2022. PMID: 34937151 Free PMC article. Review. Chinese.
Cited by
-
Preliminary exploration of the correlation between spectral computed tomography quantitative parameters and spread through air spaces in lung adenocarcinoma.Quant Imaging Med Surg. 2024 Jan 3;14(1):386-396. doi: 10.21037/qims-23-984. Epub 2023 Nov 13. Quant Imaging Med Surg. 2024. PMID: 38223127 Free PMC article.
-
Nomogram based on clinical characteristics and radiological features for the preoperative prediction of spread through air spaces in patients with clinical stage IA non-small cell lung cancer: a multicenter study.Diagn Interv Radiol. 2023 Nov 7;29(6):771-785. doi: 10.4274/dir.2023.232404. Epub 2023 Sep 19. Diagn Interv Radiol. 2023. PMID: 37724737 Free PMC article. Clinical Trial.
-
Clinical, pathological, and computed tomography morphological features of lung cancer with spread through air spaces.Transl Lung Cancer Res. 2024 Oct 31;13(10):2802-2812. doi: 10.21037/tlcr-24-715. Epub 2024 Oct 21. Transl Lung Cancer Res. 2024. PMID: 39507029 Free PMC article.
-
Performance of deep learning model and radiomics model for preoperative prediction of spread through air spaces in the surgically resected lung adenocarcinoma: a two-center comparative study.Transl Lung Cancer Res. 2024 Dec 31;13(12):3486-3499. doi: 10.21037/tlcr-24-646. Epub 2024 Dec 27. Transl Lung Cancer Res. 2024. PMID: 39830743 Free PMC article.
-
Predictive value of multiple imaging predictive models for spread through air spaces of lung adenocarcinoma: A systematic review and network meta‑analysis.Oncol Lett. 2024 Jan 25;27(3):122. doi: 10.3892/ol.2024.14255. eCollection 2024 Mar. Oncol Lett. 2024. PMID: 38348387 Free PMC article.
References
-
- Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol (2015) 10:1243–60. 10.1097/JTO.0000000000000630 - DOI - PubMed
-
- Kadota K, Nitadori J-I, Sima CS, Ujiie H, Rizk NP, Jones DR, et al. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J Thorac Oncol (2015) 10:806–14. 10.1097/JTO.0000000000000486 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources