

The Ratio of the Hemoglobin to Red Cell Distribution Width Combined with the Ratio of Platelets to Lymphocytes Can Predict the Survival of Patients with Gastric Cancer Liver Metastasis
- PMID: 33506035
- PMCID: PMC7814956
- DOI: 10.1155/2021/8729869
The Ratio of the Hemoglobin to Red Cell Distribution Width Combined with the Ratio of Platelets to Lymphocytes Can Predict the Survival of Patients with Gastric Cancer Liver Metastasis
Abstract
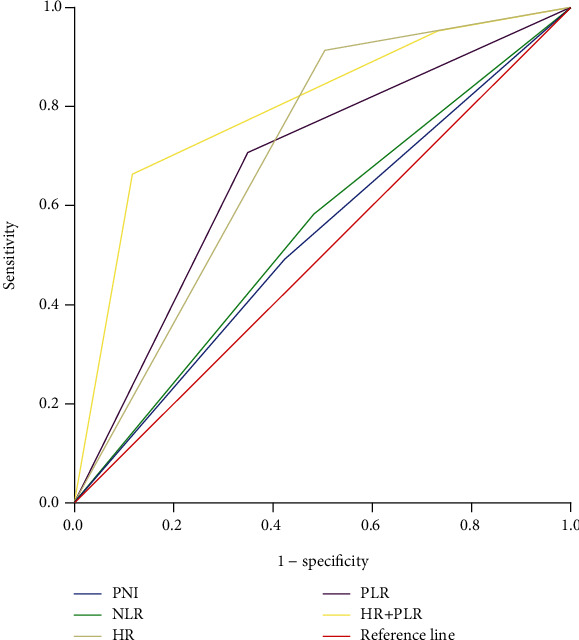
Background: Hemoglobin/red cell distribution width (HR) and platelet/lymphocyte (PLR) ratios are considered effective prognostic markers in various cancers. We have proposed a new prognostic parameter: HR+PLR. The aim of this study is to explore the prognostic value of the HR+PLR scoring system in patients with gastric cancer liver metastasis.
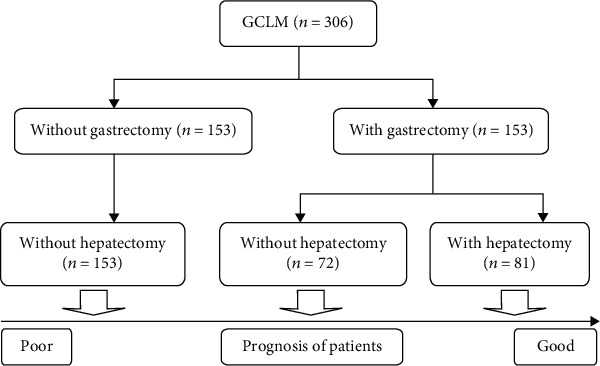
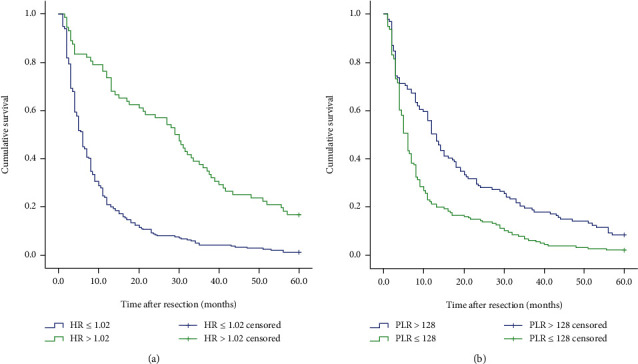
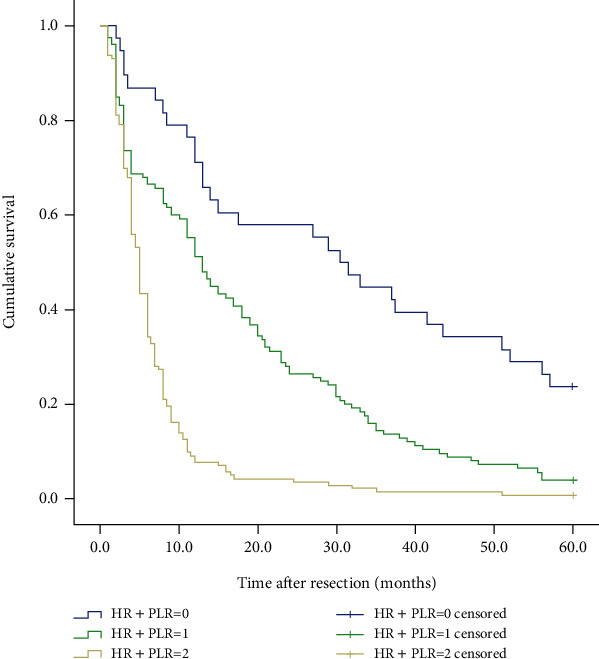
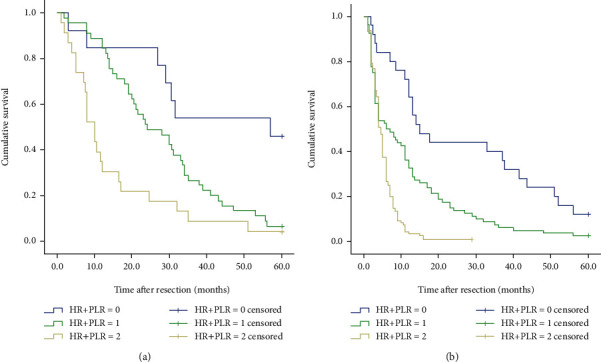
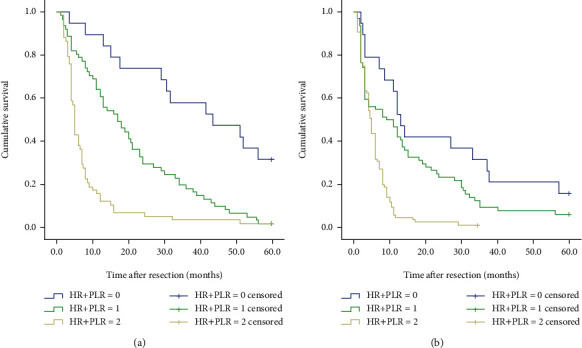
Methods: This study retrospectively analyzed the clinical data of 306 patients with gastric cancer liver metastases admitted to our hospital from 2007 to 2014. According to the size of HR value and PLR value, we will divide the patients into three groups, namely, HR+PLR: (1) 0 points: HR > 1.02 and PLR < 128; (2) 1 point: HR > 1.02 and PLR > 128 and HR < 1.02 and PLR < 128; and (3) 2 points: HR < 1.02 and PLR > 128.
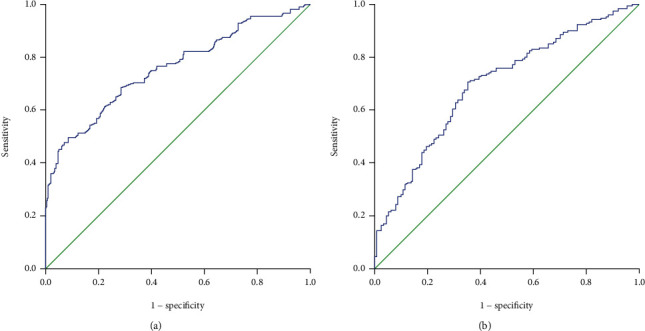
Results: The HR+PLR score was statistically different from age (P = 0.049), T stage (P < 0.001), N stage (P = 0.017), number of liver metastases (P = 0.018), gastrectomy (P < 0.001), hepatectomy (P = 0.001), peritoneal metastasis (P = 0.012), prognostic nutritional index (PNI) (P = 0.028), and neutrophil/lymphocyte ratio (NLR) (P = 0.045). The HR+PLR scoring system has a higher area under the ROC curve (AUC value) than PNI, PLR, HR, and PLR (AUC = 0.798, P < 0.001). In multivariate analysis, gastrectomy (P = 0.001), hepatectomy (P < 0.001), chemotherapy (P = 0.014), and HR+PLR score (P < 0.001) were considered independent prognostic factors.
Conclusion: For patients with gastric cancer liver metastasis, the HR+PLR score is a simple, reliable, and economic prognostic marker.
Copyright © 2021 Zhao Zhai et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Prognostic significance of the neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio in patients with metastatic gastric cancer.Medicine (Baltimore). 2020 Mar;99(10):e19405. doi: 10.1097/MD.0000000000019405. Medicine (Baltimore). 2020. PMID: 32150090 Free PMC article.
-
Preoperative Platelet-to-Lymphocyte Ratio (PLR) for Predicting the Survival of Stage I-III Gastric Cancer Patients with a MGC Component.Biomed Res Int. 2021 May 3;2021:9678363. doi: 10.1155/2021/9678363. eCollection 2021. Biomed Res Int. 2021. PMID: 33997045 Free PMC article.
-
Can the neutrophil-lymphocyte ratio and platelet-lymphocyte ratio be beneficial in predicting lymph node metastasis and promising prognostic markers of gastric cancer patients? Tumor maker retrospective study.Int J Surg. 2018 Aug;56:320-327. doi: 10.1016/j.ijsu.2018.06.037. Epub 2018 Jun 30. Int J Surg. 2018. PMID: 29969732
-
Pretreatment platelet-to-lymphocyte ratio is associated with the response to first-line chemotherapy and survival in patients with metastatic gastric cancer.J Clin Lab Anal. 2018 Jan;32(1):e22185. doi: 10.1002/jcla.22185. Epub 2017 Feb 26. J Clin Lab Anal. 2018. PMID: 28238215 Free PMC article.
-
What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP's prognostic ability in different cancer types.Oncotarget. 2023 Feb 25;14:153-172. doi: 10.18632/oncotarget.28367. Oncotarget. 2023. PMID: 36848404 Free PMC article. Review.
Cited by
-
Lower haemoglobin-to-red blood cell distribution width ratio is independently associated with frailty in community-dwelling older adults: a cross-sectional study.BMJ Open. 2023 Jul 9;13(7):e069141. doi: 10.1136/bmjopen-2022-069141. BMJ Open. 2023. PMID: 37423632 Free PMC article.
-
Predictive value of the early postoperative hemoglobin-to-red blood cell distribution width ratio for acute kidney injury in elderly intertrochanteric fracture patients.BMC Musculoskelet Disord. 2024 Aug 7;25(1):630. doi: 10.1186/s12891-024-07745-y. BMC Musculoskelet Disord. 2024. PMID: 39113005 Free PMC article.
-
C-reactive protein-to-lymphocyte ratio and hemoglobin-to-red cell distribution width ratio as effective prognostic predictors in pediatric patients with neuroblastoma.Eur J Pediatr. 2025 Jul 21;184(8):493. doi: 10.1007/s00431-025-06334-y. Eur J Pediatr. 2025. PMID: 40689991
-
Relationship between the Hemoglobin-to-Red Cell Distribution Width Ratio and All-Cause Mortality in Septic Patients with Atrial Fibrillation: Based on Propensity Score Matching Method.J Cardiovasc Dev Dis. 2022 Nov 18;9(11):400. doi: 10.3390/jcdd9110400. J Cardiovasc Dev Dis. 2022. PMID: 36421935 Free PMC article.
-
Prognostic ability of the haemoglobin-to-red blood cell distribution width ratio in predicting in-hospital mortality: a retrospective, longitudinal, observational study among elderly patients with acute ischaemic stroke.BMJ Open. 2025 Jun 22;15(6):e097075. doi: 10.1136/bmjopen-2024-097075. BMJ Open. 2025. PMID: 40545302 Free PMC article.
References
-
- Siegel R. L., Miller K. D., Jemal A. Cancer statistics, 2019. CA: a Cancer Journal for Clinicians. 2018;69(1):7–34. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
