

A pictorial review of the utility of CEUS in thoracic biopsies
- PMID: 33506348
- PMCID: PMC7840822
- DOI: 10.1186/s13244-020-00944-w
A pictorial review of the utility of CEUS in thoracic biopsies
Abstract
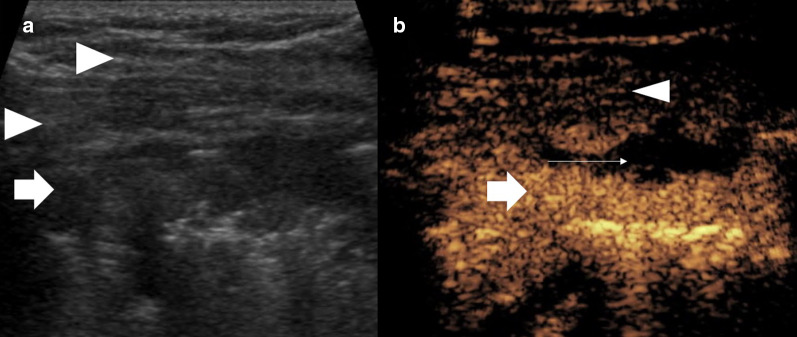
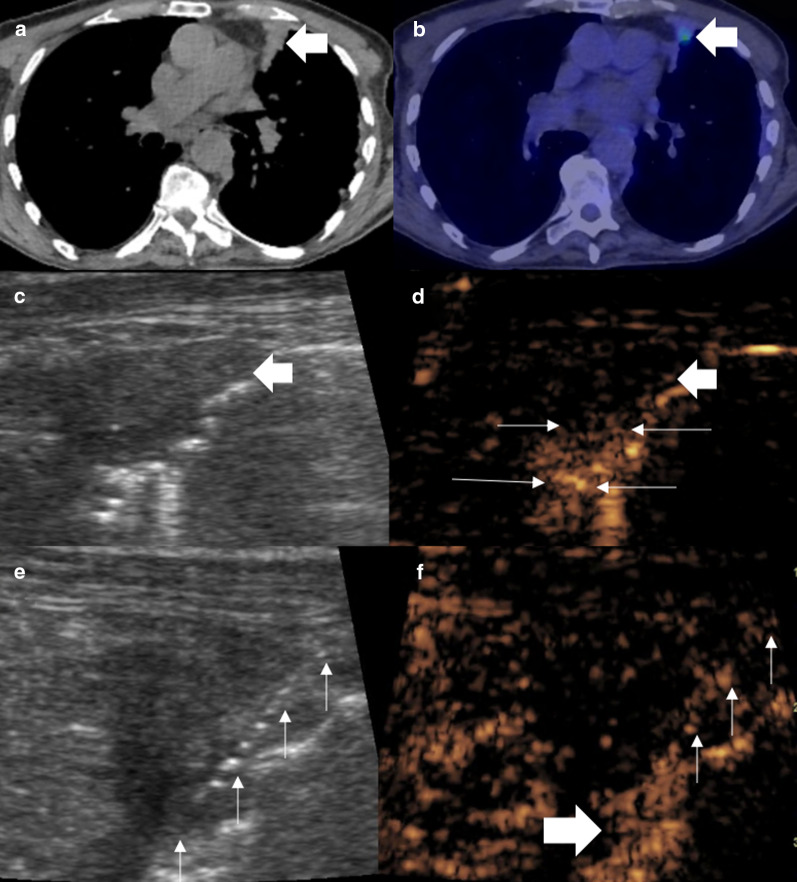
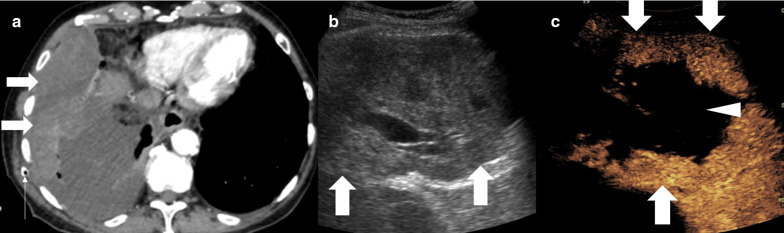
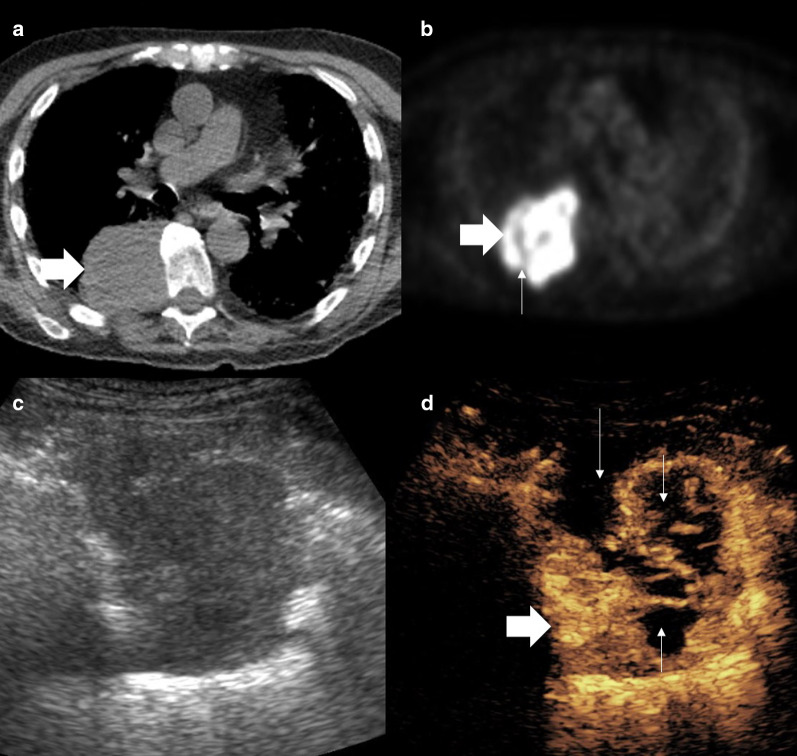
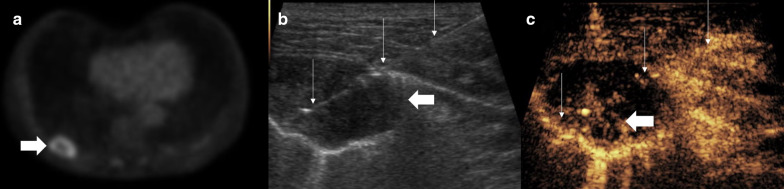
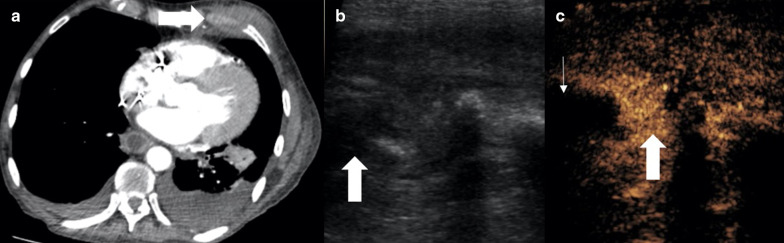
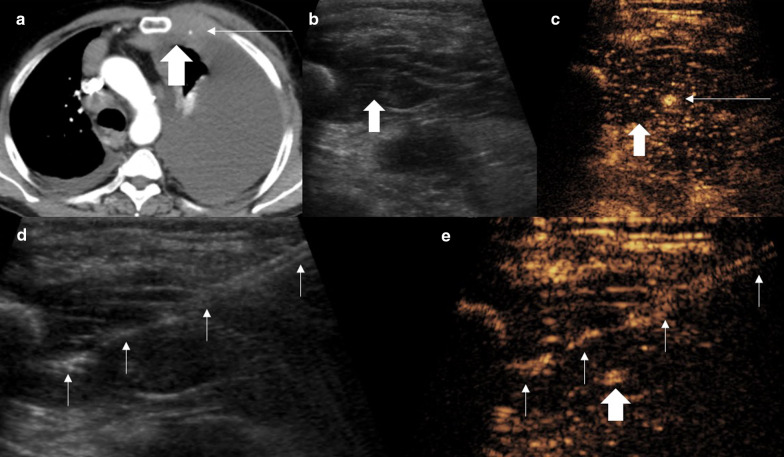
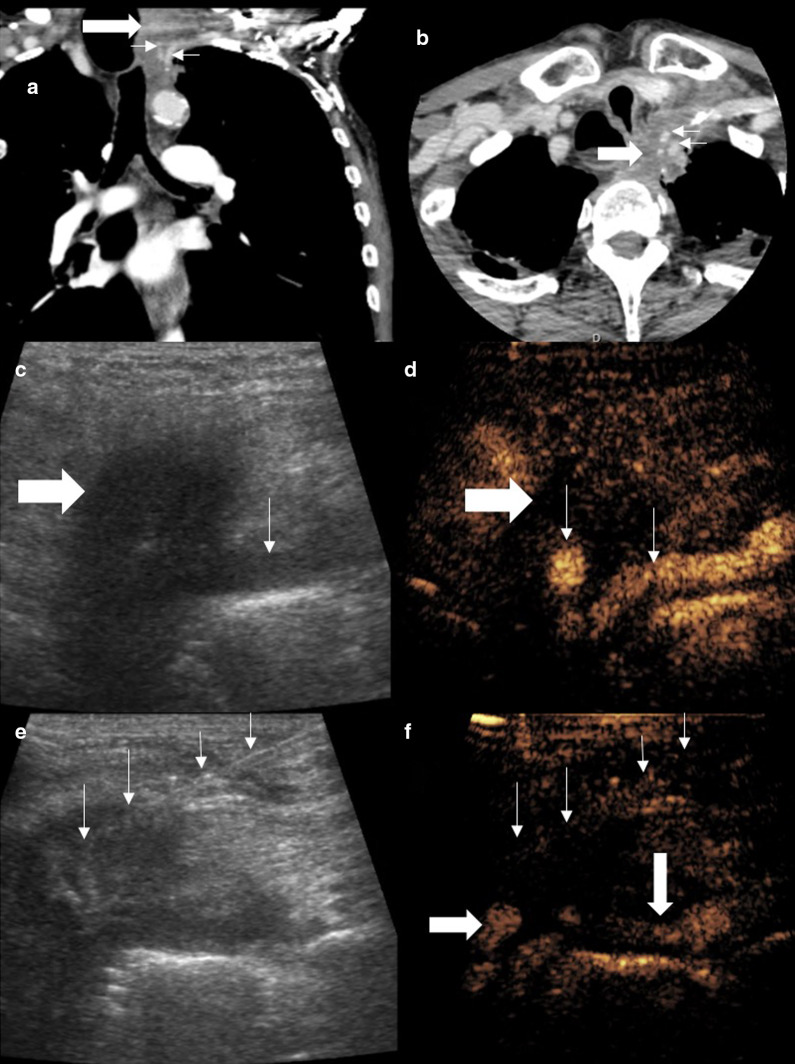
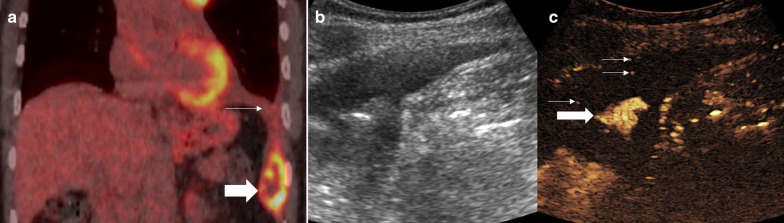
Lung cancer is one of the commonest malignancies worldwide and necessitates both early and personalised treatment. A key requirement is histological sampling with immunohistochemistry obtained usually from percutaneous biopsy. Conventionally thoracic biopsies are performed using CT guidance, but more recently, there has been development of physician led ultrasound biopsy for pleural lesions. Contrast-enhanced ultrasound (CEUS) has been increasingly used in interventional procedures and is able to offer benefits for thoracic biopsies including improving lesional visualisation and characterisation, targeting viable tissue and avoiding critical vascular structures as well as evaluating for the presence of post-procedural complications. This educational review aims to benefits of the role of CEUS in thoracic biopsies.
Keywords: Biopsy; CEUS; Contrast-enhanced ultrasound; Lung cancer; Pleural.
Conflict of interest statement
GTY has received honoraria for Siemens and Bracco. PSS has received honoraria from Siemens, Samsung, Hitachi and Bracco, and consulting fees from ITREAS. DYH, DR, SBP, KS have no disclosures.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
