

Efficacy of three-dimensional computed tomography volumetry for recipients in downsizing oversized grafts in brain-dead donor lung transplantation
- PMID: 33506436
- PMCID: PMC7840616
- DOI: 10.1007/s11748-021-01591-8
Efficacy of three-dimensional computed tomography volumetry for recipients in downsizing oversized grafts in brain-dead donor lung transplantation
Abstract
Objective: Brain-dead donor lung transplantation frequently requires reduction in the size of oversized lung grafts for patients with a small chest cavity. We focused on the role of three-dimensional computed tomography (3D-CT) volumetry for recipients on downsizing oversized lung grafts.
Methods: We performed 53 brain-dead donor bilateral lung transplantations, including 15 lobar lung transplants (Lobar group) and 38 standard lung transplants with full-sized grafts (Full group), between December 2010 and December 2018. Recipient chest volume before transplantation was measured using 3D-CT volumetry, and donor lung volume was evaluated by predicted total lung capacity. Post-transplant outcomes and pulmonary function were retrospectively compared between the groups.
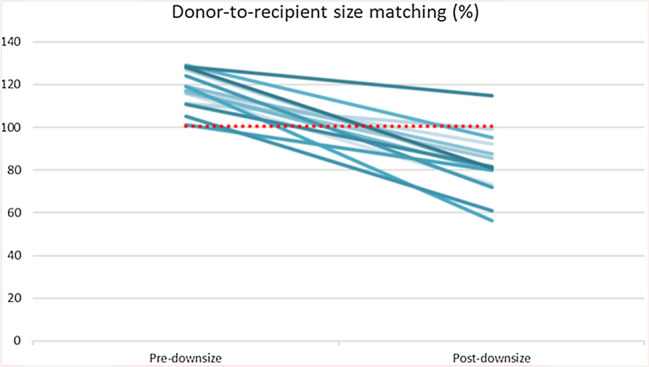
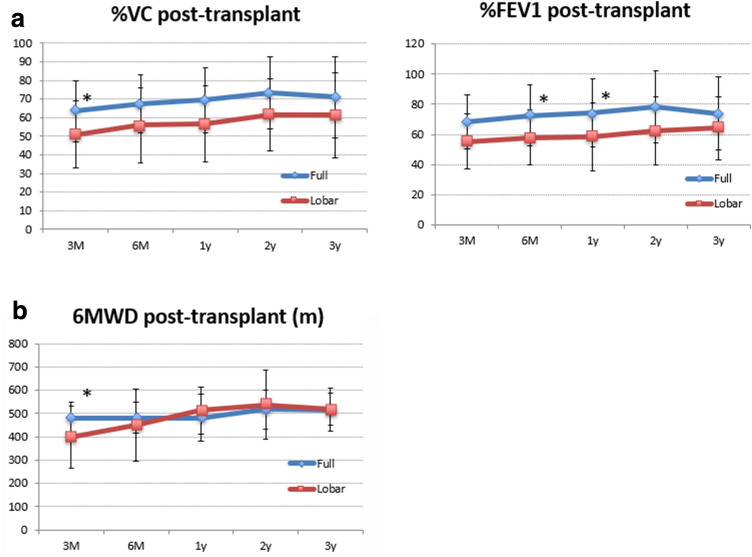
Results: The ratio of the recipient chest volume to the donor lung volume was significantly lower in the Lobar group (0.42 ± 0.15) than in the Full group (0.77 ± 0.30, P < 0.01). The calculated size matching between the donor and recipient after downsizing the grafts was significantly correlated to the ratio of the recipient chest volume to the donor lung volume (Spearman r = 0.69; P < 0.01). Early post-transplant outcomes did not significantly differ between the groups. Although the Full group showed slightly better pulmonary function after transplantation, the 1-, 3-, and 5-year overall survival rates were similar to the Lobar group (100%, 93%, and 81% in the Lobar group vs. 92%, 78%, and 70% in the Full group; P = 0.50).
Conclusions: Brain-dead donor lobar lung transplantation showed favorable post-transplant outcomes. The assessment of recipient chest cavity volume using 3D-CT volumetry may help surgeons precisely downsize oversized lung grafts prior to transplantation.
Keywords: Brain dead donor; Lobar lung transplantation; Oversized graft; Three-dimensional computed tomography volumetry.
Conflict of interest statement
All the authors have declared no competing interest.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
