

Differences in High- and Low-Value Cardiovascular Testing by Health Insurance Provider
- PMID: 33506684
- PMCID: PMC7955432
- DOI: 10.1161/JAHA.120.018877
Differences in High- and Low-Value Cardiovascular Testing by Health Insurance Provider
Abstract
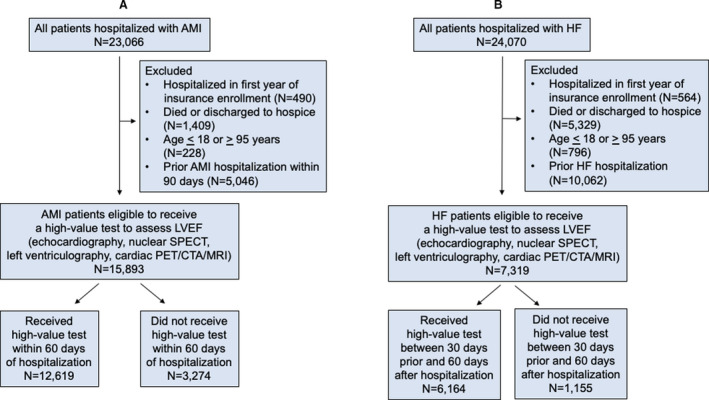
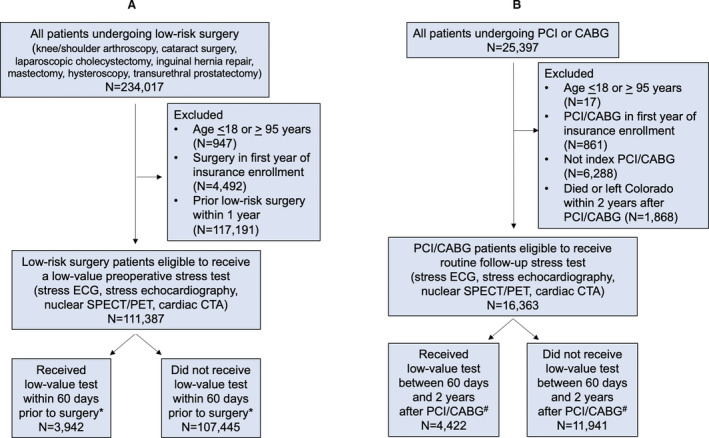
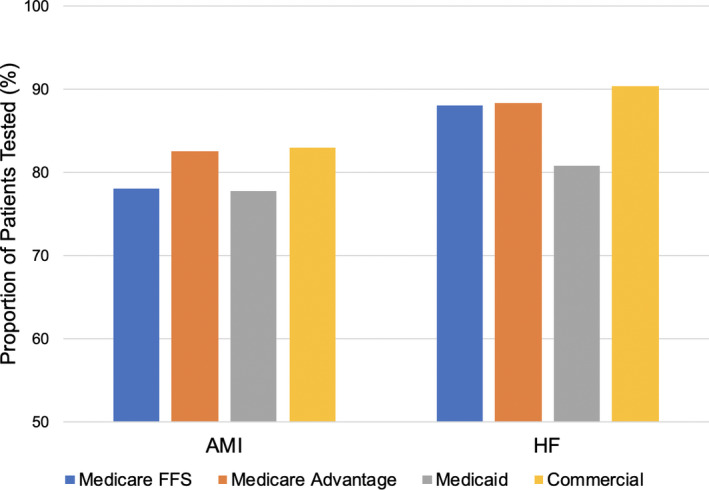
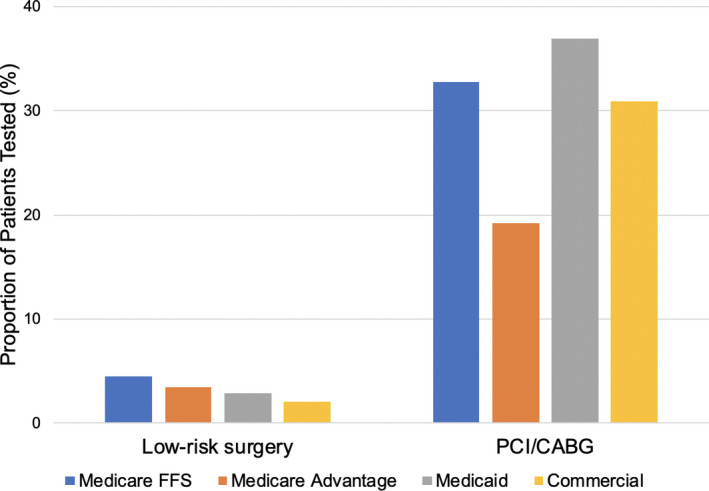
Background Quality of care incentives and reimbursements for cardiovascular testing differ between insurance providers. We hypothesized that there are differences in the use of guideline-concordant testing between Medicaid versus commercial insurance patients <65 years, and between Medicare Advantage versus Medicare fee-for-service patients ≥65 years. Methods and Results Using data from the Colorado All-Payer Claims Database from 2015 to 2018, we identified patients eligible to receive a high-value test recommended by guidelines: assessment of left ventricular function among patients hospitalized with acute myocardial infarction or incident heart failure, or a low-value test that provides minimal patient benefit: stress testing prior to low-risk surgery or routine stress testing within 2 years of percutaneous coronary intervention or coronary artery bypass graft surgery. Among 145 616 eligible patients, 37% had fee-for-service Medicare, 18% Medicare Advantage, 22% Medicaid, and 23% commercial insurance. Using multilevel logistic regression models adjusted for patient characteristics, Medicaid patients were less likely to receive high-value testing for acute myocardial infarction (odds ratio [OR], 0.84 [0.73-0.98]; P=0.03) and heart failure (OR, 0.59 [0.51-0.70]; P<0.01) compared with commercially insured patients. Medicare Advantage patients were more likely to receive high-value testing for acute myocardial infarction (OR, 1.35 [1.15-1.59]; P<0.01) and less likely to receive low-value testing after percutaneous coronary intervention/ coronary artery bypass graft (OR, 0.63 [0.55-0.72]; P<0.01) compared with Medicare fee-for-service patients. Conclusions Guideline-concordant testing was less likely to occur among patients with Medicaid compared with commercial insurance, and more likely to occur among patients with Medicare Advantage compared with fee-for-service Medicare. Insurance plan features may provide valuable targets to improve guideline-concordant testing.
Keywords: health policy; imaging; quality of care.
Conflict of interest statement
Dr Ho has a research agreement with Bristol‐Myers Squibb through the University of Colorado. He serves as the Deputy Editor for
Figures
Similar articles
-
Trends in High- and Low-Value Cardiovascular Diagnostic Testing in Fee-for-Service Medicare, 2000-2016.JAMA Netw Open. 2019 Oct 2;2(10):e1913070. doi: 10.1001/jamanetworkopen.2019.13070. JAMA Netw Open. 2019. PMID: 31603486 Free PMC article.
-
Trends in US Ambulatory Care Patterns During the COVID-19 Pandemic, 2019-2021.JAMA. 2022 Jan 18;327(3):237-247. doi: 10.1001/jama.2021.24294. JAMA. 2022. PMID: 35040886 Free PMC article.
-
The effect of cost-containment policies on rates of coronary revascularization in California.N Engl J Med. 1993 Dec 9;329(24):1784-9. doi: 10.1056/NEJM199312093292407. N Engl J Med. 1993. PMID: 8232488
-
Government and private insurance medical programs as well as MDVIP, an update.J Long Term Eff Med Implants. 2004;14(3):243-50. doi: 10.1615/jlongtermeffmedimplants.v14.i3.80. J Long Term Eff Med Implants. 2004. PMID: 15301667 Review.
-
The Medicare Appropriate Use Criteria Program: A Review of Recommendations for Testing in Coronary Artery Disease.Ann Intern Med. 2023 Sep;176(9):1235-1239. doi: 10.7326/M23-1011. Epub 2023 Aug 22. Ann Intern Med. 2023. PMID: 37603865 Review.
Cited by
-
2024 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.Circulation. 2024 Feb 20;149(8):e347-e913. doi: 10.1161/CIR.0000000000001209. Epub 2024 Jan 24. Circulation. 2024. PMID: 38264914 Free PMC article. Review.
-
Strategies to Reduce Low-Value Cardiovascular Care: A Scientific Statement From the American Heart Association.Circ Cardiovasc Qual Outcomes. 2022 Mar;15(3):e000105. doi: 10.1161/HCQ.0000000000000105. Epub 2022 Feb 22. Circ Cardiovasc Qual Outcomes. 2022. PMID: 35189687 Free PMC article. Review.
-
Patient Symptoms and Stress Testing After Elective Percutaneous Coronary Intervention in the Veterans Affairs Health Care System.JAMA Netw Open. 2022 Jun 1;5(6):e2217704. doi: 10.1001/jamanetworkopen.2022.17704. JAMA Netw Open. 2022. PMID: 35727581 Free PMC article.
-
2025 Heart Disease and Stroke Statistics: A Report of US and Global Data From the American Heart Association.Circulation. 2025 Feb 25;151(8):e41-e660. doi: 10.1161/CIR.0000000000001303. Epub 2025 Jan 27. Circulation. 2025. PMID: 39866113 Review.
-
Associations of Chinese diagnosis-related group system with low-value coronary revascularisation: an interrupted time series analysis.BMJ Open. 2025 Mar 22;15(3):e087165. doi: 10.1136/bmjopen-2024-087165. BMJ Open. 2025. PMID: 40122549 Free PMC article.
References
-
- Mark DB, Anderson JL, Brinker JA, Brophy JA, Casey DE, Cross RR, Edmundowicz D, Hachamovitch R, Hlatky MA, Jacobs JE, et al. ACC/AHA/ASE/ASNC/HRS/IAC/Mended Hearts/NASCI/RSNA/SAIP/SCAI/SCCT/SCMR/SNMMI 2014 health policy statement on use of noninvasive cardiovascular imaging: a report of the American College of Cardiology Clinical Quality Committee. J Am Coll Cardiol. 2014;63:698–721. DOI: 10.1016/j.jacc.2013.02.002. - DOI - PubMed
-
- Safavi KC, Li SX, Dharmarajan K, Venkatesh AK, Strait KM, Lin H, Lowe TJ, Fazel R, Nallamothu BK, Krumholz HM. Hospital variation in the use of noninvasive cardiac imaging and its association with downstream testing, interventions, and outcomes. JAMA Intern Med. 2014;174:546–553. DOI: 10.1001/jamainternmed.2013.14407 - DOI - PMC - PubMed
-
- Wolk MJ, Bailey SR, Doherty JU, Douglas PS, Hendel RC, Kramer CM, Min JK, Patel MR, Rosenbaum L, Shaw LJ, et al. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease. J Am Coll Cardiol. 2014;63:380–406. DOI: 10.1016/j.jacc.2013.11.009 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
