

Major risk factors and histopathological profile of treatment failure, relapse and chronic patients with anthroponotic cutaneous leishmaniasis: A prospective case-control study on treatment outcome and their medical importance
- PMID: 33507940
- PMCID: PMC7872302
- DOI: 10.1371/journal.pntd.0009089
Major risk factors and histopathological profile of treatment failure, relapse and chronic patients with anthroponotic cutaneous leishmaniasis: A prospective case-control study on treatment outcome and their medical importance
Abstract
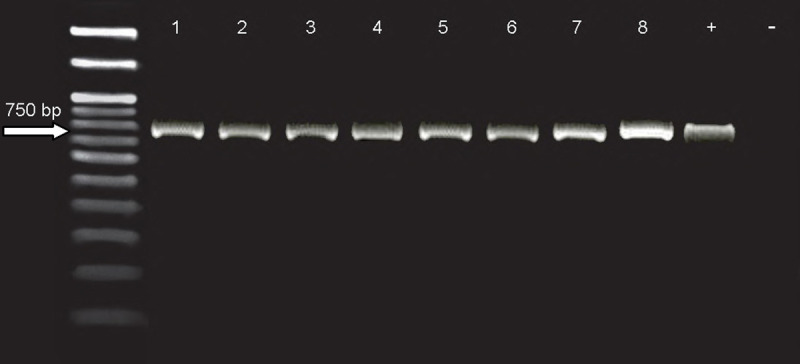
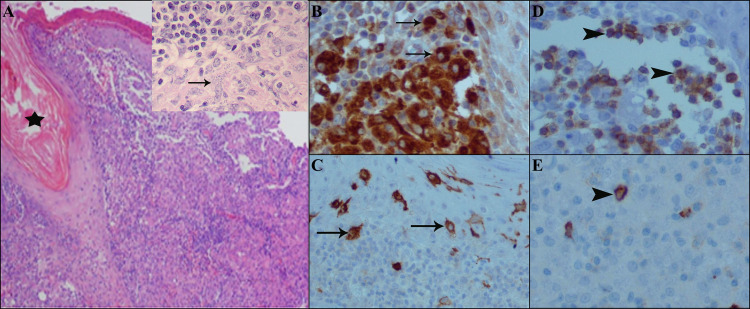
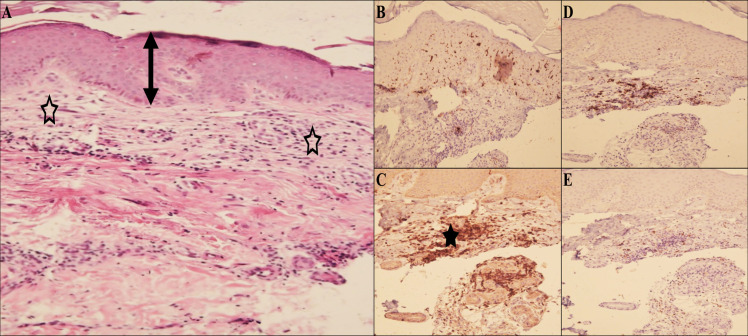
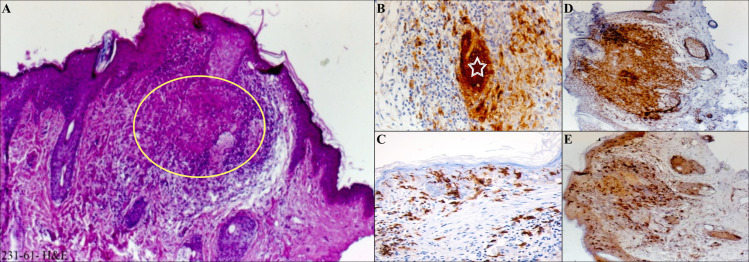
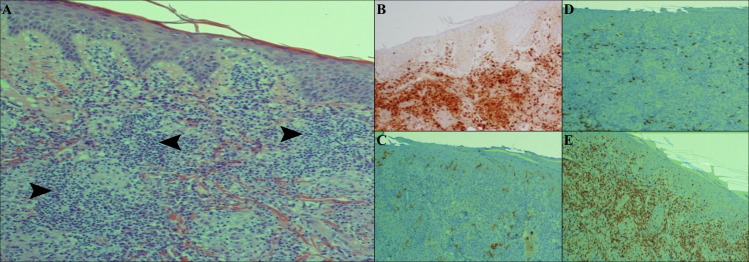
Over the last years, there has been a remarkable increase in the number of unresponsive patients with anthroponotic cutaneous leishmaniasis (ACL) reported worldwide. The primary objective of this study was to explore the role of demographic, clinical and environmental risk related-factors in the development of treatment failure, relapse and chronic cases compared to responsive patients with ACL. Moreover, molecular, histopathological and immunohistochemical (IHC) findings between these forms were explored. This work was undertaken as a prospective and case-control study in southeastern Iran. Culture media and nested PCR were used to identify the causative agent. Univariate multinomial and multiple multinomial logistic regression models and the backward elimination stepwise method were applied to analyze the data. A P<0.05 was defined as significant. Also, for different groups, skin punch biopsies were used to study the histopathological and immunohistochemical (IHC) profile. All samples showed that L. tropica was the only etiological agent in all unresponsive and responsive patients with ACL. Data analysis represented that 8 major risk factors including nationality, age groups, occupation, marital status, history of chronic diseases, duration of the lesion, the lesion on face and presence of domestic animals in the house were significantly associated with the induction of unresponsive forms. The histopathological and immunohistochemical findings were different from one form to another. The present findings clearly demonstrated a positive relation between ACL and distinct demographic, clinical and environmental risk determinants. Knowledge of the main risk factors for ACL infection is crucial in improving clinical and public health strategies and monitor such perplexing factors.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Risk factors for anthroponotic cutaneous leishmaniasis in unresponsive and responsive patients in a major focus, southeast of Iran.PLoS One. 2018 Feb 7;13(2):e0192236. doi: 10.1371/journal.pone.0192236. eCollection 2018. PLoS One. 2018. PMID: 29415078 Free PMC article.
-
Associated-risk determinants for anthroponotic cutaneous leishmaniasis treated with meglumine antimoniate: A cohort study in Iran.PLoS Negl Trop Dis. 2019 Jun 12;13(6):e0007423. doi: 10.1371/journal.pntd.0007423. eCollection 2019 Jun. PLoS Negl Trop Dis. 2019. PMID: 31188834 Free PMC article.
-
Host's immune response in unresponsive and responsive patients with anthroponotic cutaneous leishmaniasis treated by meglumine antimoniate: A case-control study of Th1 and Th2 pathways.Int Immunopharmacol. 2019 Apr;69:321-327. doi: 10.1016/j.intimp.2019.02.008. Epub 2019 Feb 14. Int Immunopharmacol. 2019. PMID: 30771740
-
Changes in the Epidemiology of Cutaneous Leishmaniasis in Northeastern Iran.Turkiye Parazitol Derg. 2020 Mar 20;44(1):52-57. doi: 10.4274/tpd.galenos.2019.6137. Turkiye Parazitol Derg. 2020. PMID: 32212595 Review.
-
Determinants of Unresponsiveness to Treatment in Cutaneous Leishmaniasis: A Focus on Anthroponotic Form Due to Leishmania tropica.Front Microbiol. 2021 Jun 1;12:638957. doi: 10.3389/fmicb.2021.638957. eCollection 2021. Front Microbiol. 2021. PMID: 34140933 Free PMC article. Review.
Cited by
-
Systematic Review of Treatment Failure and Clinical Relapses in Leishmaniasis from a Multifactorial Perspective: Clinical Aspects, Factors Associated with the Parasite and Host.Trop Med Infect Dis. 2023 Aug 29;8(9):430. doi: 10.3390/tropicalmed8090430. Trop Med Infect Dis. 2023. PMID: 37755891 Free PMC article. Review.
-
Fifty years of struggle to control cutaneous leishmaniasis in the highest endemic county in Iran: A longitudinal observation inferred with interrupted time series model.PLoS Negl Trop Dis. 2022 Apr 29;16(4):e0010271. doi: 10.1371/journal.pntd.0010271. eCollection 2022 Apr. PLoS Negl Trop Dis. 2022. PMID: 35486645 Free PMC article.
-
Clinical Profile and Diagnosis of Recurrent Cutaneous Leishmaniasis.Open Forum Infect Dis. 2023 Jul 22;10(8):ofad387. doi: 10.1093/ofid/ofad387. eCollection 2023 Aug. Open Forum Infect Dis. 2023. PMID: 37564745 Free PMC article.
-
The developing role of NRF2 and HMOX1 in treatment response of cutaneous leishmaniasis.Sci Rep. 2025 Apr 29;15(1):14988. doi: 10.1038/s41598-025-99456-0. Sci Rep. 2025. PMID: 40301619 Free PMC article.
-
Geographical and climatic risk factors of cutaneous leishmaniasis in the hyper-endemic focus of Bam County in southeast Iran.Front Public Health. 2023 Nov 9;11:1236552. doi: 10.3389/fpubh.2023.1236552. eCollection 2023. Front Public Health. 2023. PMID: 38026324 Free PMC article.
References
-
- WHO, Organization WH. Control of the leishmaniases: report of a meeting of the WHO expert committee on the control of leishmaniases. Control of the leishmaniases: report of a meeting of the WHO expert committee on the control of leishmaniases. Geneva: World Health Organization; 2010. pp. 1–187.
-
- Ponte-Sucre A, Diaz E, Padrón-Nieves M. Drug Resistance in Leishmania Parasites: Consequences, Molecular Mechanisms and Possible Treatments. Springer Science & Business Media; 2012.
-
- WHO. Global Health Observatory data repository: Number of cases of cutaneous leishmaniasis reported. 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
