

Comparison of different cardiovascular risk tools used in HIV patient cohorts in sub-Saharan Africa; do we need to include laboratory tests?
- PMID: 33507945
- PMCID: PMC7842918
- DOI: 10.1371/journal.pone.0243552
Comparison of different cardiovascular risk tools used in HIV patient cohorts in sub-Saharan Africa; do we need to include laboratory tests?
Abstract
Introduction: Cardiovascular disease (CVD) is the leading cause of death globally, representing 31% of all global deaths. HIV and long term anti-retroviral therapy (ART) are risk factors for development of CVD in populations of people living with HIV (PLHIV). CVD risk assessment tools are currently being applied to SSA populations, but there are questions about accuracy as well as implementation challenges of these tools in lower resource setting populations. We aimed to assess the level of agreement between the various cardiovascular screening tools (Data collection on Adverse effects of anti-HIV Drugs (D:A:D), Framingham risk score, WHO risk score and The Atherosclerotic Cardiovascular Disease Score) when applied to an HIV ART experienced population in Sub-Saharan Africa.
Methods: This study was undertaken in an Anti-Retroviral Long Term (ALT) Cohort of 1000 PLHIV in care who have been on ART for at least 10 years in urban Uganda. A systematic review was undertaken to find the most frequently used screening tools from SSA PLHIV populations; these were applied to the ALT cohort. Levels of agreement between the resulting scores (those including lipids and non-lipids based, as well as HIV-specific and non-HIV specific) as applied to our cohort were compared. Prevalence Bias Adjusted Kappa was used to evaluate agreement between tools.
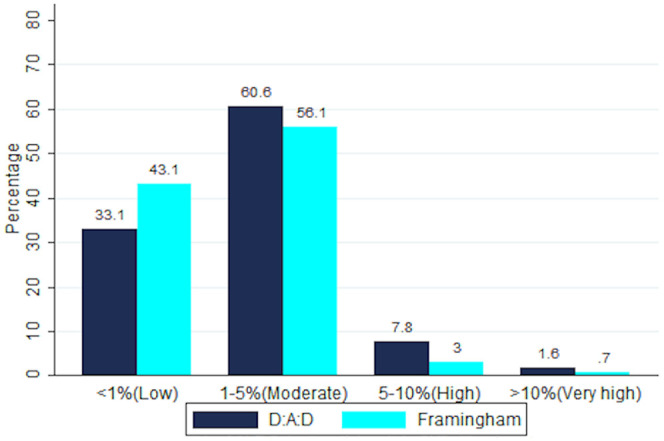
Results: Overall, PLHIV in ALT cohort had a median score of 1.1-1.4% risk of a CVD event over 5 years and 1.7-2.5% risk of a CVD event over 10 years. There was no statistical difference in the risk scores obtained for this population when comparing the different tools, including comparisons of those with lipids and non-lipids, and HIV specific vs non-HIV specific.
Conclusion: The various tools yielded similar results, but those not including lipids are more feasible to apply in our setting. Long-term cohorts of PLHIV in SSA should in future provide longitudinal data to evaluate existing CVD risk prediction tools for these populations. Inclusion of HIV and ART history factors to existing scoring systems may improve accuracy without adding the expense and technical difficulty of lipid testing.
Conflict of interest statement
The study was funded in part (SJR) by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health and Janssen pharmaceutical company through Johnson & Johnson corporate citizenship trust. There are no patents, products in development or marketed products to declare. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Cardiovascular risk factors in HIV infected individuals: Comparison with general adult control population in Greece.PLoS One. 2020 Mar 30;15(3):e0230730. doi: 10.1371/journal.pone.0230730. eCollection 2020. PLoS One. 2020. PMID: 32226048 Free PMC article.
-
Assessing the impact of antiretroviral therapy on tuberculosis notification rates among people with HIV: a descriptive analysis of 23 countries in sub-Saharan Africa, 2010-2015.BMC Infect Dis. 2018 Sep 26;18(1):481. doi: 10.1186/s12879-018-3387-z. BMC Infect Dis. 2018. PMID: 30257667 Free PMC article.
-
The association between antiretroviral therapy and selected cardiovascular disease risk factors in sub-Saharan Africa: A systematic review and meta-analysis.PLoS One. 2018 Jul 30;13(7):e0201404. doi: 10.1371/journal.pone.0201404. eCollection 2018. PLoS One. 2018. PMID: 30059546 Free PMC article.
-
Reaching the 'first 90': Gaps in coverage of HIV testing among people living with HIV in 16 African countries.PLoS One. 2017 Oct 12;12(10):e0186316. doi: 10.1371/journal.pone.0186316. eCollection 2017. PLoS One. 2017. PMID: 29023510 Free PMC article.
-
Prevalence, Risk Factors, and Pathophysiology of Dysglycemia among People Living with HIV in Sub-Saharan Africa.J Diabetes Res. 2018 May 23;2018:6916497. doi: 10.1155/2018/6916497. eCollection 2018. J Diabetes Res. 2018. PMID: 30009182 Free PMC article. Review.
Cited by
-
Prevalence and incidence of hypertension in a heavily treatment-experienced cohort of people living with HIV in Uganda.PLoS One. 2023 Feb 17;18(2):e0282001. doi: 10.1371/journal.pone.0282001. eCollection 2023. PLoS One. 2023. PMID: 36800379 Free PMC article.
-
Evaluation of Cardiovascular Risk Profile and Risk Scores of Antiretroviral Therapy-naïve HIV Patients in Eastern India.J Glob Infect Dis. 2024 Aug 7;16(3):104-110. doi: 10.4103/jgid.jgid_29_24. eCollection 2024 Jul-Sep. J Glob Infect Dis. 2024. PMID: 39619366 Free PMC article.
-
Comparative performance of cardiovascular risk prediction models in people living with HIV.South Afr J HIV Med. 2022 Nov 15;23(1):1395. doi: 10.4102/sajhivmed.v23i1.1395. eCollection 2022. South Afr J HIV Med. 2022. PMID: 36479421 Free PMC article.
-
Predicting the risk of atherosclerotic cardiovascular disease among adults living with HIV/AIDS in Addis Ababa, Ethiopia: A hospital-based study.PLoS One. 2021 Nov 29;16(11):e0260109. doi: 10.1371/journal.pone.0260109. eCollection 2021. PLoS One. 2021. PMID: 34843544 Free PMC article.
-
Comparison of Predicted Cardiovascular Risk Profiles by Different CVD Risk-Scoring Algorithms between HIV-1-Infected and Uninfected Adults: A Cross-Sectional Study in Tanzania.HIV AIDS (Auckl). 2021 Jun 3;13:605-615. doi: 10.2147/HIV.S304982. eCollection 2021. HIV AIDS (Auckl). 2021. PMID: 34113177 Free PMC article.
References
-
- WHO. Non---Communicable Disease Risk Factor Baseline Survey UGANDA Geneva; 2016.
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984–2008. Am J Epidemiol. 2013;177(2):116–25. 10.1093/aje/kws321 - DOI - PMC - PubMed
-
- Dwomoh D, Tambaa C, Ayisi Addo S, Wiah E, Abdulai M, Bosomprah S. Effect of antiretroviral therapy on all-cause mortality among people living with HIV/AIDS in Ghana using Mahalanobis distant metric matching within propensity score caliper analysis: A retrospective cohort study. PLoS One. 2018;13(9):e0203461 10.1371/journal.pone.0203461 - DOI - PMC - PubMed
-
- Kasamba I, Baisley K, Mayanja BN, Maher D, Grosskurth H. The impact of antiretroviral treatment on mortality trends of HIV-positive adults in rural Uganda: a longitudinal population-based study, 1999–2009. Tropical medicine & international health: TM & IH. 2012;17(8):e66–73. 10.1111/j.1365-3156.2012.02841.x - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
