

High-dose corticosteroid pulse therapy increases the survival rate in COVID-19 patients at risk of hyper-inflammatory response
- PMID: 33507958
- PMCID: PMC7842890
- DOI: 10.1371/journal.pone.0243964
High-dose corticosteroid pulse therapy increases the survival rate in COVID-19 patients at risk of hyper-inflammatory response
Abstract
Objective: Test whether high dose corticosteroid pulse therapy (HDCPT) with either methylprednisolone or dexamethasone is associated with increased survival in COVID-19 patients at risk of hyper-inflammatory response. Provide some initial diagnostic criteria using laboratory markers to stratify these patients.
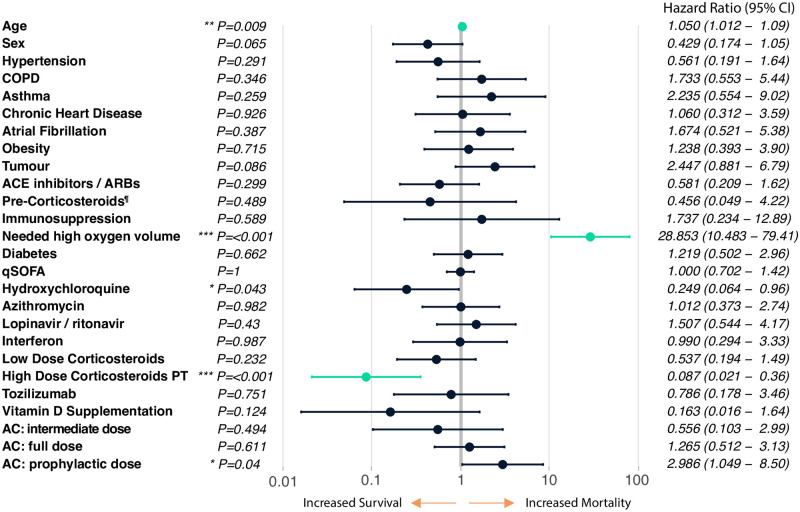
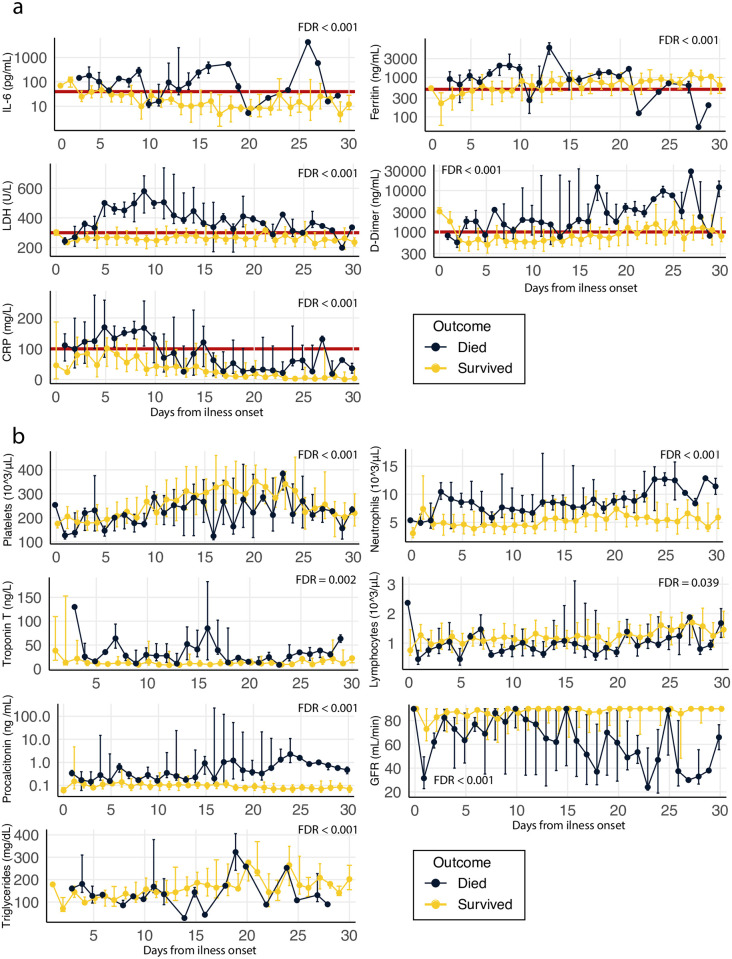
Methods: This is a prospective observational study, 318 met the inclusion criteria. 64 patients (20.1%) were treated with HDCPT by using at least 1.5mg/kg/24h of methylprednisolone or dexamethasone equivalent. A multivariate Cox regression (controlling for co-morbidities and other therapies) was carried out to determine whether HDCPT (among other interventions) was associated with decreased mortality. We also carried out a 30-day time course analysis of laboratory markers between survivors and non-survivors, to identify potential markers for patient stratification.
Results: HDCPT showed a statistically significant decrease in mortality (HR = 0.087 [95% CI 0.021-0.36]; P < 0.001). 30-day time course analysis of laboratory marker tests showed marked differences in pro-inflammatory markers between survivors and non-survivors. As diagnostic criteria to define the patients at risk of developing a COVID-19 hyper-inflammatory response, we propose the following parameters (IL-6 > = 40 pg/ml, and/or two of the following: C-reactive protein > = 100 mg/L, D-dimer > = 1000 ng/ml, ferritin > = 500 ng/ml and lactate dehydrogenase > = 300 U/L).
Conclusions: HDCPT can be an effective intervention to increase COVID-19 survival rates in patients at risk of developing a COVID-19 hyper-inflammatory response, laboratory marker tests can be used to stratify these patients who should be given HDCPT. This study is not a randomized clinical trial (RCT). Future RCTs should be carried out to confirm the efficacy of HDCPT to increase the survival rates of COVID-19.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
