

Atrial fibrillation burden and heart failure: Data from 39,710 individuals with cardiac implanted electronic devices
- PMID: 33508517
- PMCID: PMC8096675
- DOI: 10.1016/j.hrthm.2021.01.021
Atrial fibrillation burden and heart failure: Data from 39,710 individuals with cardiac implanted electronic devices
Abstract
Background: Atrial fibrillation (AF) and heart failure (HF) often accompany one another, and each is independently associated with poor outcomes. However, the association between AF burden and outcomes is poorly understood.
Objective: The purpose of this study was to describe the association between device-based AF burden and HF clinical outcomes.
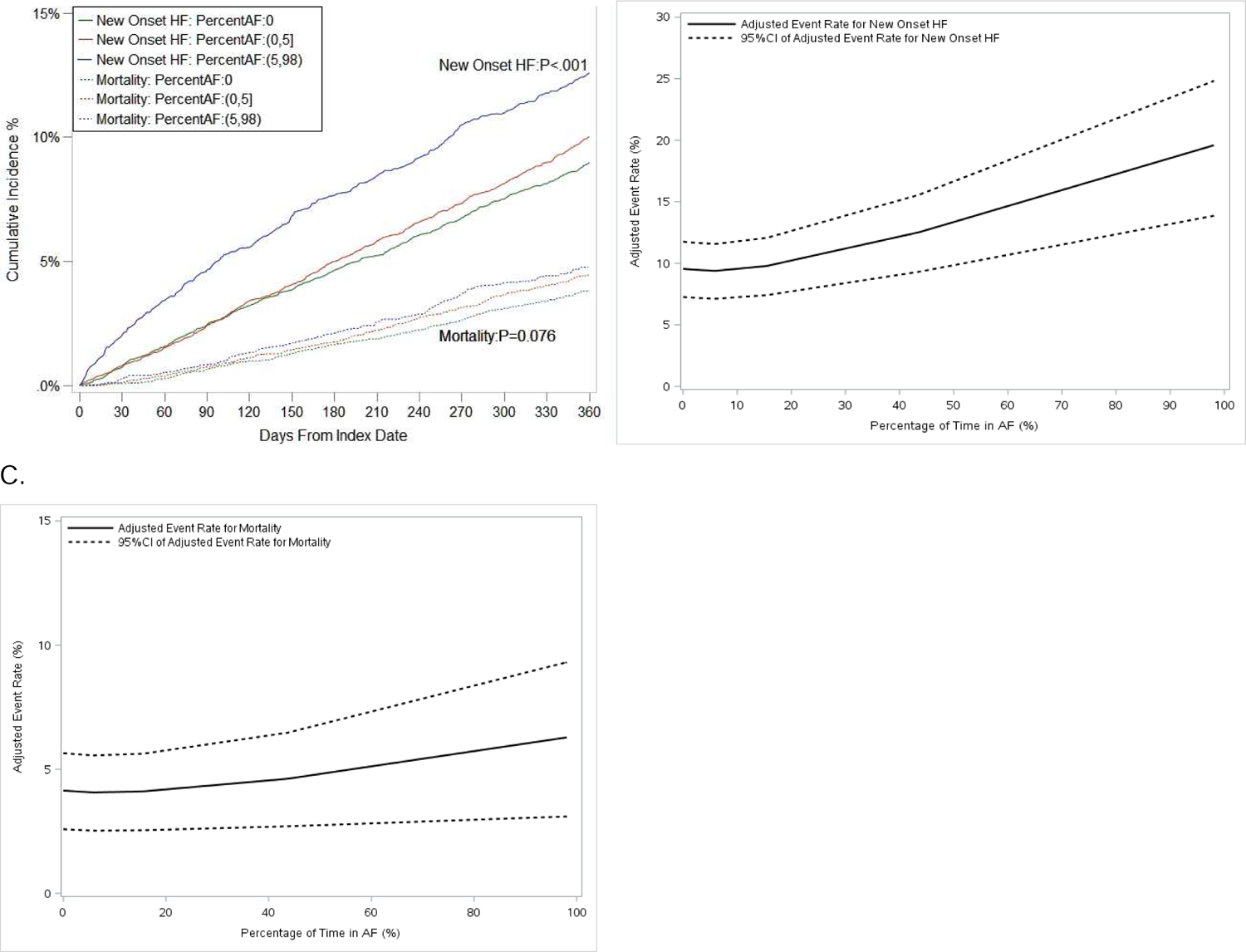
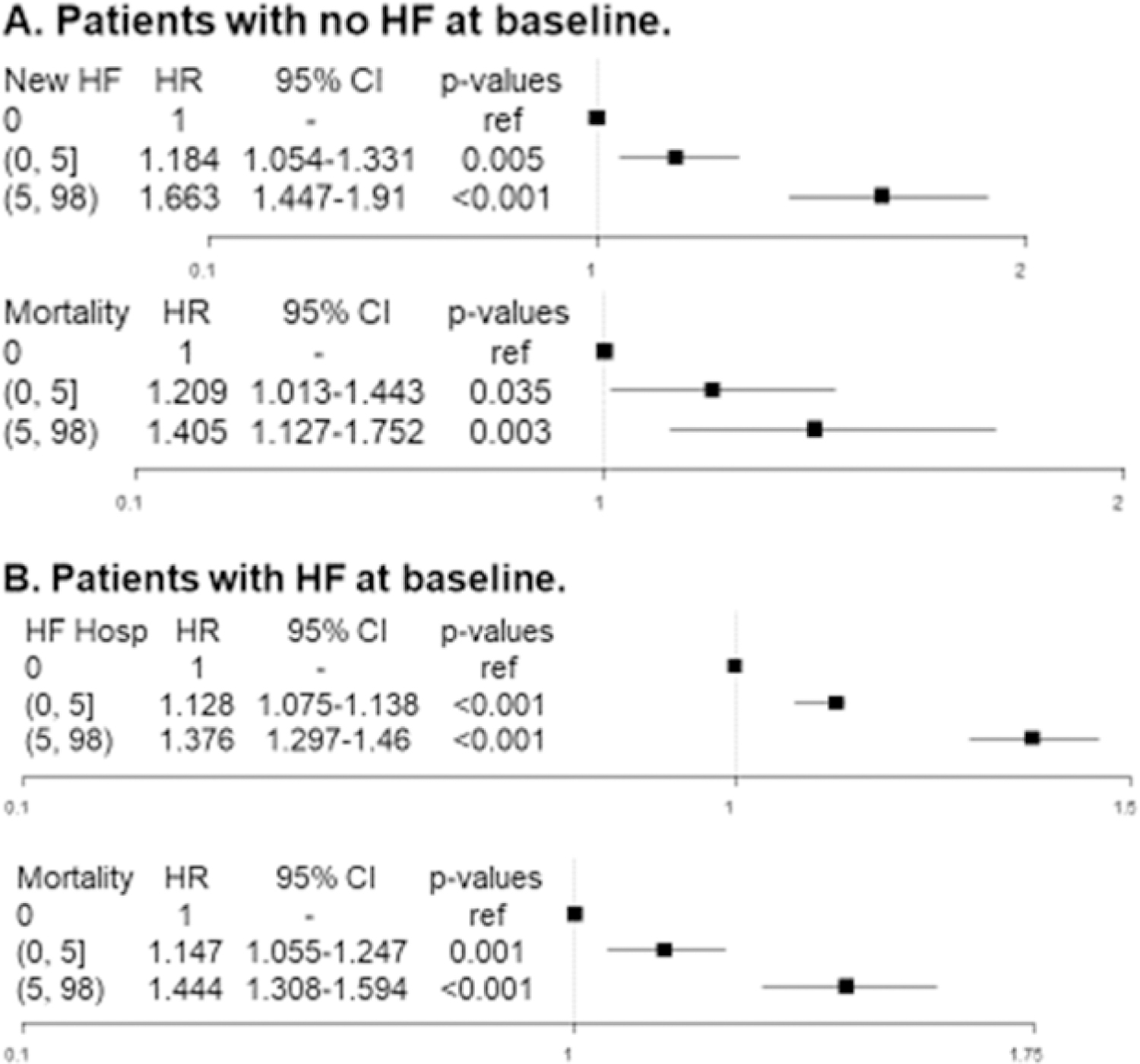
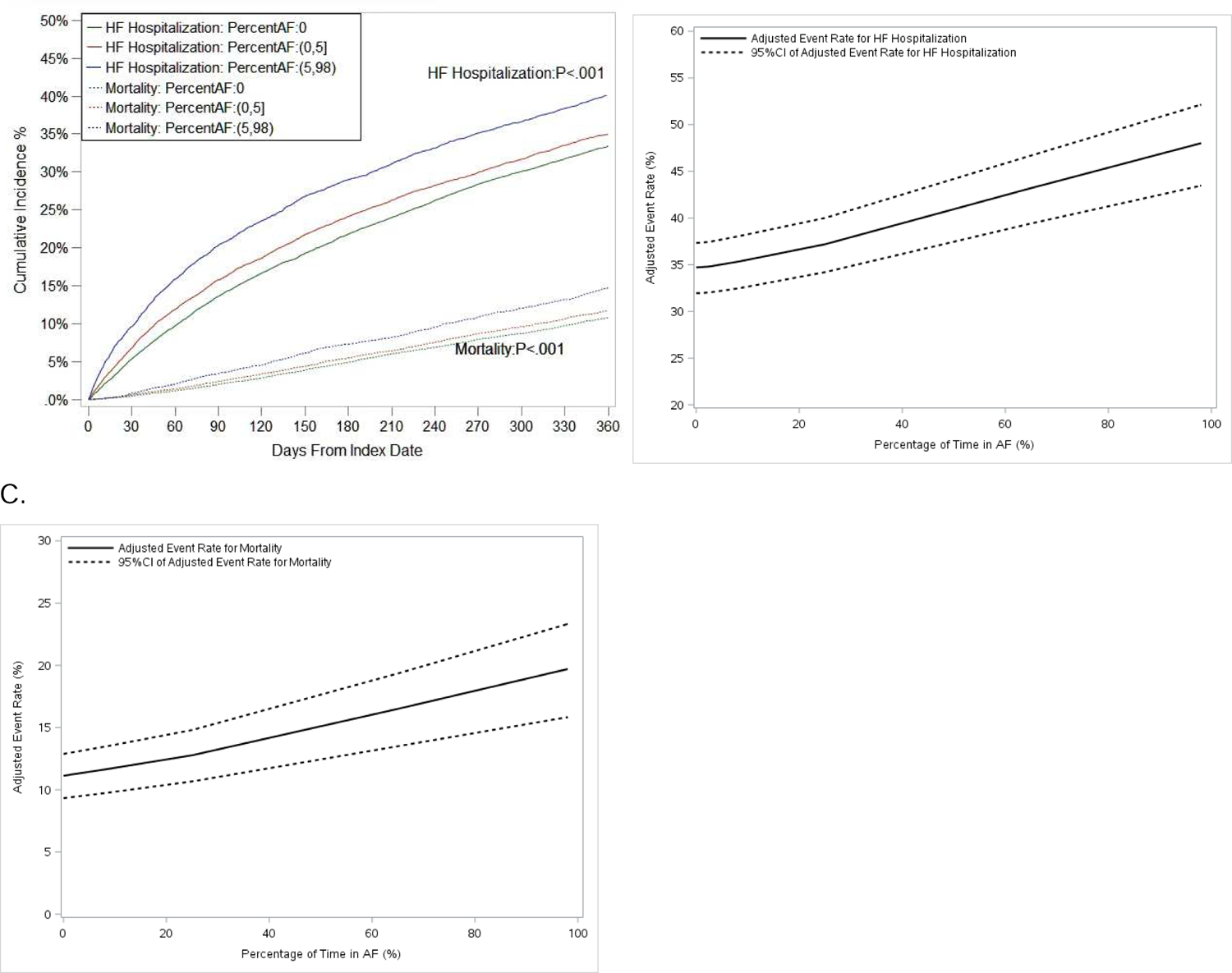
Methods: We used a nationwide, remote monitoring database of cardiac implantable electronic devices (CIEDs) linked to Medicare claims. We included patients with nonpermanent AF, undergoing new CIED implant, stratified by baseline HF. The outcomes were new-onset HF, HF hospitalization, and all-cause mortality at 1 and 3 years.
Results: We identified 39,710 patients who met inclusion criteria (25,054 with HF; 14,656 without HF). Patients with HF were younger (mean age 76.3 vs 78.5 years; P <.001), more often male (65% vs 54%; P <.001), and had higher mean CHA2DS2-VASc scores (5.4 vs 4.1; P <.001). Among those without HF, increasing device-based AF burden was significantly associated with increased risk of new-onset HF (adjusted hazard ratio [HR] 1.09 per 10% AF burden; 95% confidence interval [CI] 1.06-1.12; P <.001) and all-cause mortality (adjusted HR 1.05 per 10% AF burden; 95% CI 1.01-1.10; P = .012). Among patients with HF, increasing AF burden was significantly associated with increased risk of HF hospitalization (adjusted HR 1.05 per 10% AF burden; 95% CI 1.04-1.06; P <.001) and all-cause mortality (adjusted HR 1.06 per 10% AF burden; 95% CI 1.05-1.08; P <.001).
Conclusion: Among older patients with AF receiving a CIED, increasing AF burden is significantly associated with increasing risk of adverse HF outcomes and all-cause mortality.
Keywords: Arrhythmia burden; Atrial fibrillation; Heart failure; Medicare; Outcomes; Remote monitoring.
Copyright © 2021 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wolf PA, Dawber TR, Thomas HE Jr., Kannel WB. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham study. Neurology 1978;28:973–977. - PubMed
-
- Nieuwlaat R, Prins MH, Le Heuzey JY, et al. Prognosis, disease progression, and treatment of atrial fibrillation patients during 1 year: follow-up of the Euro Heart Survey on atrial fibrillation. Eur Heart J 2008;29:1181–1189. - PubMed
-
- Steinberg BA, Piccini JP. When Low-Risk Atrial Fibrillation Is Not So Low Risk: Beast of Burden. JAMA cardiology 2018;3:558–560. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
