Rapid Symptom Improvement in Major Depressive Disorder Using Accelerated Repetitive Transcranial Magnetic Stimulation
- PMID: 33508790
- PMCID: PMC7851468
- DOI: 10.9758/cpn.2021.19.1.73
Rapid Symptom Improvement in Major Depressive Disorder Using Accelerated Repetitive Transcranial Magnetic Stimulation
Abstract
Objective: Repetitive transcranial magnetic stimulation (rTMS) has contributed to increase in the remission rate for patients with major depressive disorder (MDD). However, current rTMS treatment is practically inconvenient because it requires daily treatment sessions for several weeks. Accelerated rTMS treatment is as efficient and safe for MDD patients as conventional rTMS.
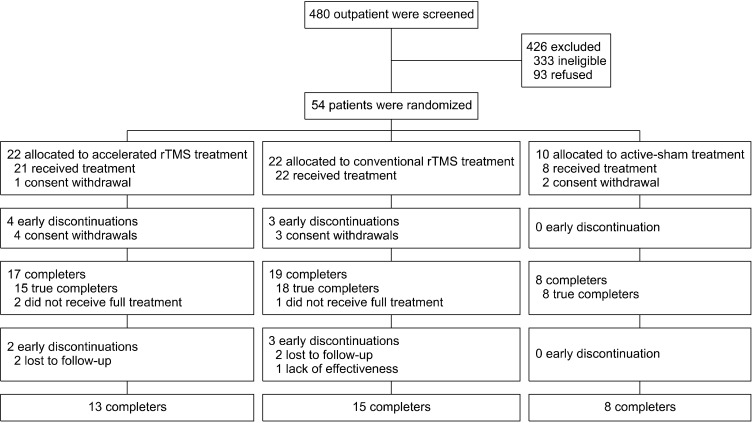
Methods: Fifty-one patients with MDD participated in this study; they were randomized into accelerated rTMS (n = 21), conventional rTMS (n = 22), and sham-treatment (n = 8) groups. The accelerated and conventional rTMS groups received 15 sessions for 3 days and 3 weeks, respectively. The sham-treatment group received 15 sham rTMS sessions for 3 days. Primary outcome was assessed using self-report and clinician-rated Korean Quick Inventory of Depressive Symptomatology (KQIDS-SR and KQIDS-C, respectively). Adverse effects were monitored using the Frequency, Intensity, and Burden of Side Effects Rating scale. Changes in depressive symptoms were compared among the three groups using mixed model analyses.
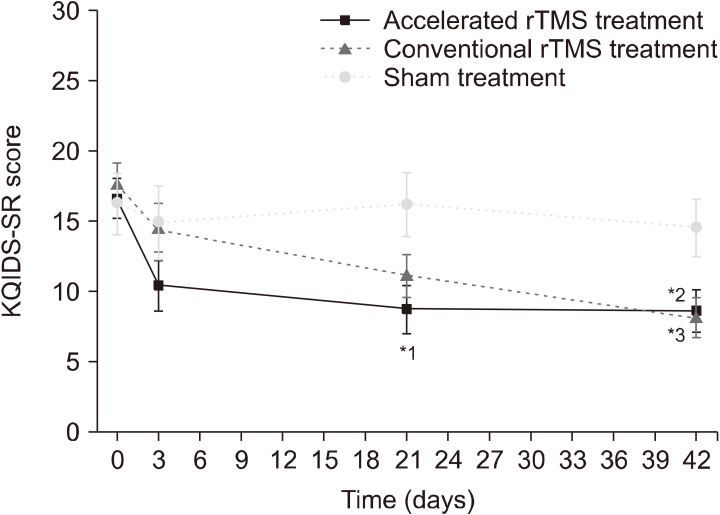
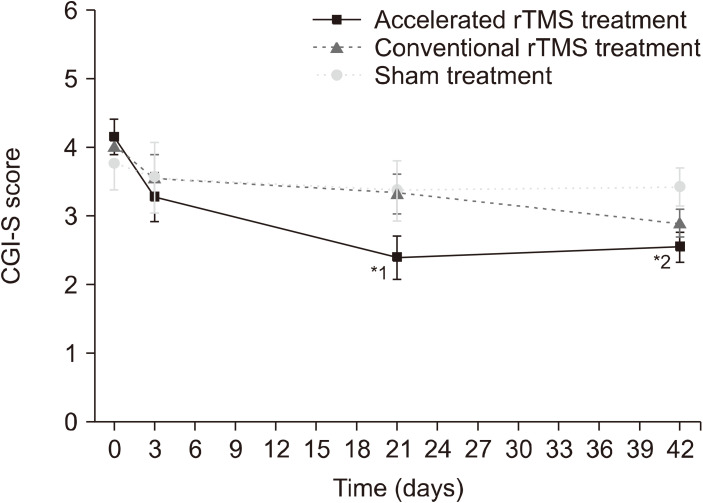
Results: For the KQIDS-SR score, there was a significant main effect of "time" (F3,47 = 11.05, p < 0.001), but no effect of "group" (F2,47 = 2.04, p = 0.142), and a trend-level interaction effect of "group × time" (F6,47 = 2.26, p = 0.053). Improvement in depressive symptoms, based on the KQIDS-SR score 3 weeks after treatment, was more prominent in the accelerated rTMS group than in the sham-treatment group (p = 0.011). Tolerability was comparable among the three groups.
Conclusion: The accelerated rTMS treatment group showed rapid improvement of depressive symptoms compared with the sham-treatment and conventional rTMS treatment groups. Therefore, accelerated rTMS treatment could be a viable option for MDD, with improved accessibility.
Keywords: Accessibility; Effectiveness; Major depressive disorder; Safety; Transcranial magnetic stimulation; health services; repetitive; treatment.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- World Health Organization, author. Preventing suicide: a global imperative. World Health Organization; Geneva: 2014.
-
- World Health Organization, author. Mental health action plan 2013-2020. World Health Organization; Geneva: 2013. p. 48.
-
- Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, et al. ; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) JAMA. 2003;289:3095–3105. - PubMed
-
- Srisurapanont M, Hong JP, Tian-Mei S, Hatim A, Liu CY, Udomratn P, et al. ; MD RAN. Clinical features of depression in Asia: results of a large prospective, cross-sectional study. Asia Pac Psychiatry. 2013;5:259–267. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous