

The future of retinal gene therapy: evolving from subretinal to intravitreal vector delivery
- PMID: 33510064
- PMCID: PMC8328774
- DOI: 10.4103/1673-5374.306063
The future of retinal gene therapy: evolving from subretinal to intravitreal vector delivery
Abstract
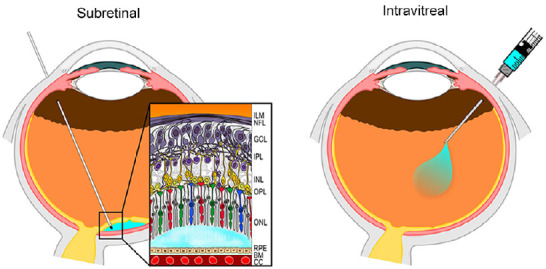
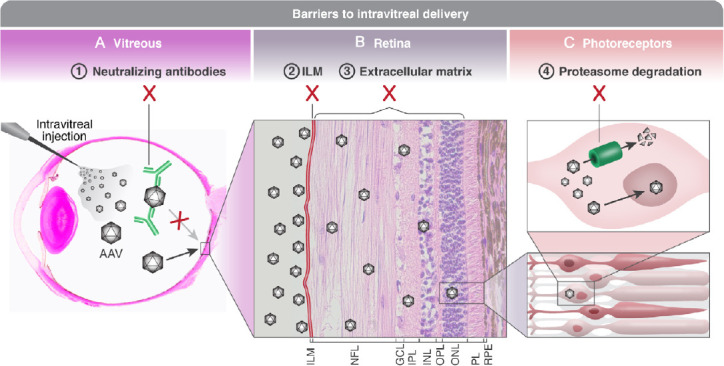
Inherited retinal degenerations are a leading and untreatbale cause of blindness, and as such they are targets for gene therapy. Numerous gene therapy treatments have progressed from laboratory research to clinical trails, and a pioneering gene therapy received the first ever FDA approval for treating patients. However, currently retinal gene therapy mostly involves subretinal injection of the therapeutic agent, which treats a limited area, entails retinal detachment and other potential complications, and requires general anesthesia with consequent risks, costs and prolonged recovery. Therefore there is great impetus to develop safer, less invasive and cheapter methods of gene delivery. A promising method is intravitreal injection, that does not cause retinal detachment, can lead to pan-retinal transduction and can be performed under local anesthesia in out-patient clinics. Intravitreally-injected vectors face several obstacles. First, the vector is diluted by the vitreous and has to overcome a long diffusion distance to the target cells. Second, the vector is exposed to the host's immune response, risking neutralization by pre-existing antibodies and triggering a stronger immune response to the injection. Third, the vector has to cross the inner limiting membrane which is both a physical and a biological barrier as it contains binding sites that could cause the vector's sequestration. Finally, in the target cell the vector is prone to proteasome degradation before delivering the transgene to the nucleus. Strategies to overcome these obstacles include modifications of the viral capsid, through rational design or directed evolution, which allow resistance to the immune system, enhancement of penetration through the inner limiting membrane or reduced degradation by intracellular proteasomes. Furthermore, physical and chemical manipulations of the inner limiting membrane and vitreous aim to improve vector penetration. Finally, compact non-viral vectors that can overcome the immunological, physical and anatomical and barriers have been developed. This paper reviews ongoing efforts to develop novel, safe and efficacious methods for intravitreal delivery of therapeutic genes for inherited retinal degenerations. To date, the most promising results are achieved in rodents with robust, pan-retinal transduction following intravitreal delivery. Trials in larger animal models demonstrate transduction mostly of inner retinal layers. Despite ongoing efforts, currently no intravitreally-injected vector has demonstrated outer retinal transduction efficacy comparable to that of subretinal delivery. Further work is warranted to test promising new viral and non-viral vectors on large animal models of inherited retinal degenerations. Positive results will pave the way to development of the next generation of treatments for inherited retinal degeneration.
Keywords: adeno-associated virus; animal model; blindness; gene therapy; inner limiting membrane; photoreceptors; retina; retinitis pigmentosa; vitreous.
Conflict of interest statement
None
Figures
Similar articles
-
Evaluation of Photoreceptor Transduction Efficacy of Capsid-Modified Adeno-Associated Viral Vectors Following Intravitreal and Subretinal Delivery in Sheep.Hum Gene Ther. 2020 Jul;31(13-14):719-729. doi: 10.1089/hum.2020.023. Epub 2020 Jul 6. Hum Gene Ther. 2020. PMID: 32486858
-
SubILM Injection of AAV for Gene Delivery to the Retina.Methods Mol Biol. 2019;1950:249-262. doi: 10.1007/978-1-4939-9139-6_14. Methods Mol Biol. 2019. PMID: 30783978 Free PMC article.
-
Heparan Sulfate Binding Promotes Accumulation of Intravitreally Delivered Adeno-associated Viral Vectors at the Retina for Enhanced Transduction but Weakly Influences Tropism.J Virol. 2016 Oct 14;90(21):9878-9888. doi: 10.1128/JVI.01568-16. Print 2016 Nov 1. J Virol. 2016. PMID: 27558418 Free PMC article.
-
Suprachoroidal Delivery of Viral and Nonviral Gene Therapy for Retinal Diseases.J Ocul Pharmacol Ther. 2020 Jul/Aug;36(6):384-392. doi: 10.1089/jop.2019.0126. Epub 2020 Apr 7. J Ocul Pharmacol Ther. 2020. PMID: 32255727 Free PMC article. Review.
-
Gene therapy for inherited retinal diseases: progress and possibilities.Clin Exp Optom. 2021 May;104(4):444-454. doi: 10.1080/08164622.2021.1880863. Epub 2021 Mar 2. Clin Exp Optom. 2021. PMID: 33689657 Review.
Cited by
-
Advances in technical methods and applications of subretinal injections in experimental animals.Front Vet Sci. 2025 Apr 30;12:1574519. doi: 10.3389/fvets.2025.1574519. eCollection 2025. Front Vet Sci. 2025. PMID: 40370828 Free PMC article. Review.
-
Characterization of anti-AAV2 neutralizing antibody levels in sheep prior to and following intravitreal AAV2.7m8 injection.Gene Ther. 2024 Nov;31(11-12):580-586. doi: 10.1038/s41434-024-00495-5. Epub 2024 Oct 29. Gene Ther. 2024. PMID: 39472677 Free PMC article.
-
Intravitreal therapy-success stories and challenges.Wien Med Wochenschr. 2025 May;175(7-8):162-174. doi: 10.1007/s10354-024-01070-8. Epub 2025 Mar 3. Wien Med Wochenschr. 2025. PMID: 40029473 Free PMC article. Review.
-
Adeno-Associated Virus Vectors in Retinal Gene Therapy: Challenges, Innovations, and Future Directions.Biomolecules. 2025 Jun 28;15(7):940. doi: 10.3390/biom15070940. Biomolecules. 2025. PMID: 40723812 Free PMC article. Review.
-
Effect of degeneration stage on non-viral tissue transfection of rd10 retina ex vivo.Mol Ther Nucleic Acids. 2025 Jul 1;36(3):102616. doi: 10.1016/j.omtn.2025.102616. eCollection 2025 Sep 9. Mol Ther Nucleic Acids. 2025. PMID: 40704026 Free PMC article.
References
-
- Ali RR, Reichel MB, De Alwis M, Kanuga N, Kinnon C, Levinsky RJ, Hunt DM, Bhattacharya SS, Thrasher AJ. Adeno-associated virus gene transfer to mouse retina. Hum Gene Ther. 1998;9:81–86. - PubMed
-
- Bordet T, Behar-Cohen F. Ocular gene therapies in clinical practice: viral vectors and nonviral alternatives. Drug Discov Today. 2019;24:1685–1693. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
