

Granulomatosis with polyangiitis presenting as a solitary renal mass: A case report with imaging and literature review
- PMID: 33510827
- PMCID: PMC7815982
- DOI: 10.1016/j.radcr.2021.01.014
Granulomatosis with polyangiitis presenting as a solitary renal mass: A case report with imaging and literature review
Erratum in
-
Erratum regarding missing declaration of competing interest and patient consent statements in previously published articles.Radiol Case Rep. 2023 Jan 25;18(4):1643-1644. doi: 10.1016/j.radcr.2023.01.017. eCollection 2023 Apr. Radiol Case Rep. 2023. PMID: 36895588 Free PMC article.
Abstract
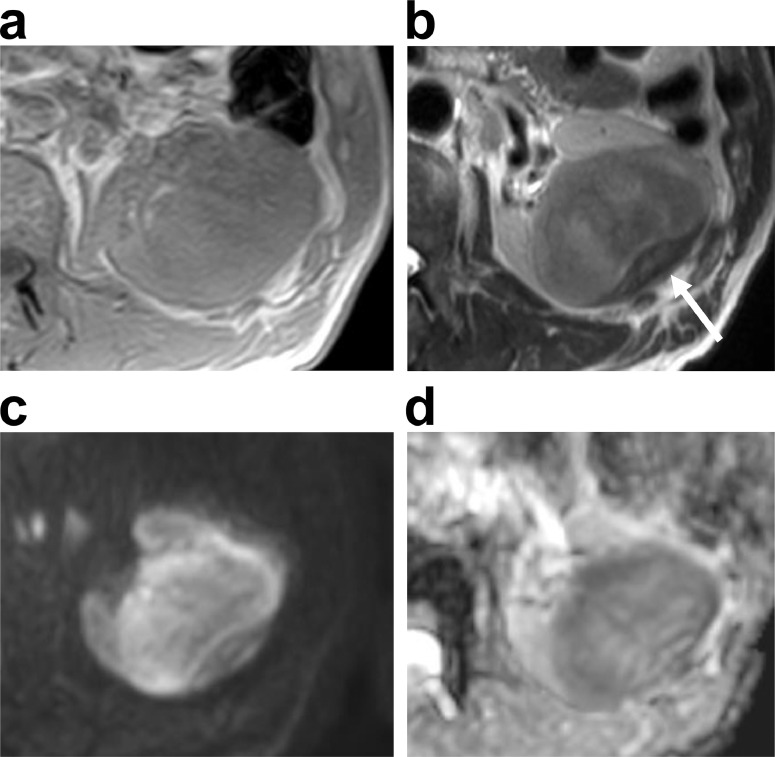
Granulomatosis with polyangiitis (GPA) manifests as necrotizing granulomatous inflammatory masses in the nasal cavity, paranasal sinuses, and lungs. However, a mass in the kidney is extremely rare. We herein report a case of GPA that presented as a solitary mass in the left kidney. The patient was a man in his 60s. A 2.5-cm solitary mass was incidentally discovered in the left kidney at another hospital and was followed-up. Eight months later, the mass had enlarged, and the patient visited our hospital for further examination and treatment. The mass was hypovascular, with unclear margins on contrast-enhanced computed tomography (CT). The signal of the mass was nonuniform and iso- to slightly hypo-intense on T2-weighted and diffusion-weighted magnetic resonance imaging (MRI). Enlarged para-aortic lymph nodes were also detected on the CT and MRI. Based on imaging, malignant tumors were suspected, and nephrectomy was performed. The pathological diagnosis was GPA. We performed a literature review of this rare renal manifestation and present a summary of reported imaging findings. If a hypovascular renal mass with an unclear margin can be found in those with GPA, unnecessary operations may be avoided by actively promoting renal biopsy.
Keywords: CT; Granulomatosis with polyangiitis; Hypovascular renal mass; MRI.
© 2021 The Authors. Published by Elsevier Inc. on behalf of University of Washington.
Figures



References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
