

Neoadjuvant EGFR-TKI Therapy for EGFR-Mutant NSCLC: A Systematic Review and Pooled Analysis of Five Prospective Clinical Trials
- PMID: 33511076
- PMCID: PMC7837071
- DOI: 10.3389/fonc.2020.586596
Neoadjuvant EGFR-TKI Therapy for EGFR-Mutant NSCLC: A Systematic Review and Pooled Analysis of Five Prospective Clinical Trials
Abstract
Purpose: The role of neoadjuvant epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitor (TKI) targeted therapy for patients with EGFR-mutant non-small cell lung cancer (NSCLC) has not been clarified. A pooled analysis of prospective clinical trials was conducted to evaluate the efficacy and safety of neoadjuvant EGFR-TKI therapy.
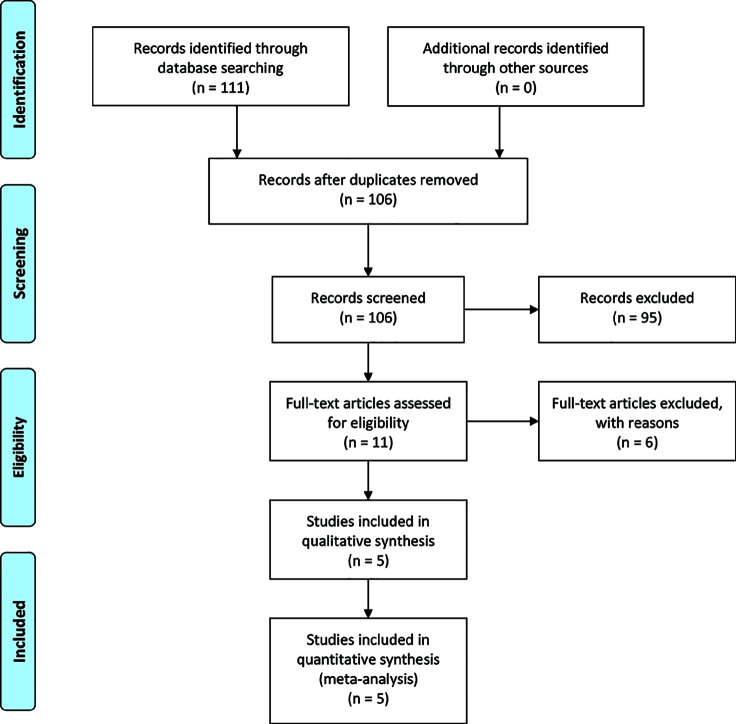
Methods: The PubMed, Embase, Web of Science, and Cochrane Library databases, as well as meeting abstracts were searched for prospective clinical trials evaluating the efficacy and safety of neoadjuvant EGFR-TKI for treatment of EGFR-mutant NSCLC. The main outcomes included the objective response rate (ORR), downstaging rate, surgical resection rate (SRR), pathologic complete response (pCR) rate, progression-free survival (PFS), and adverse events.
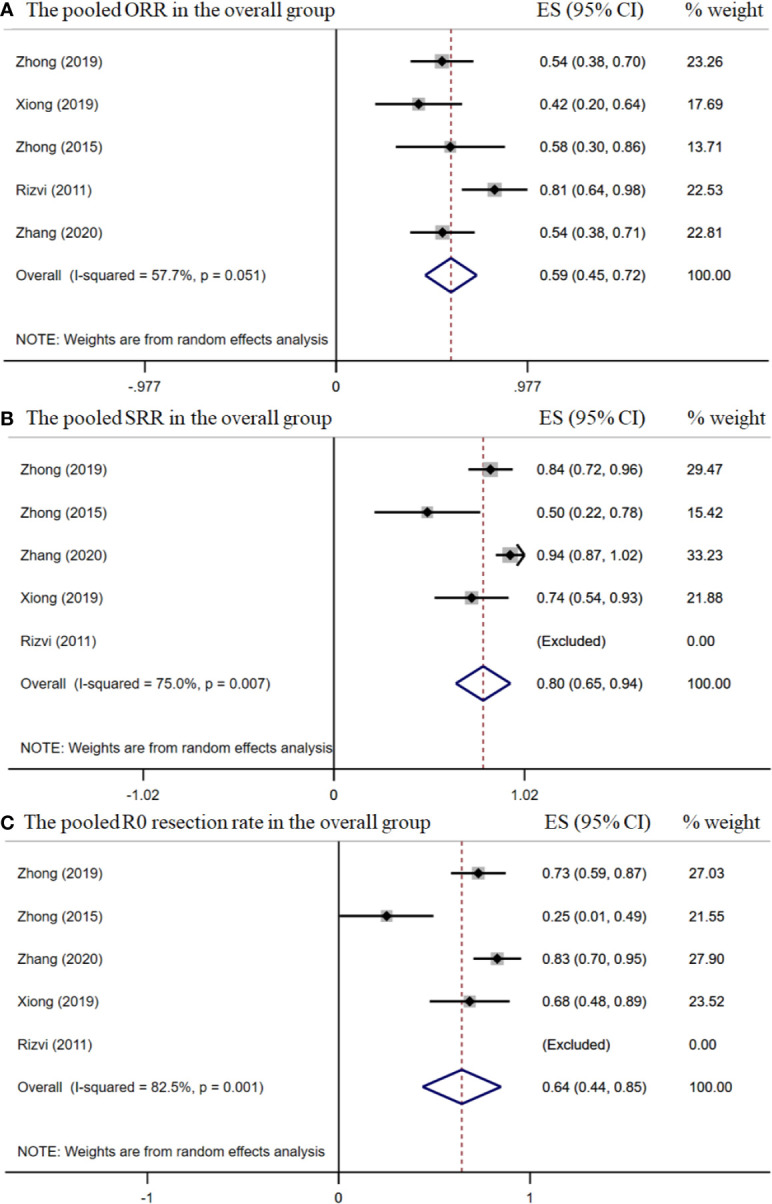
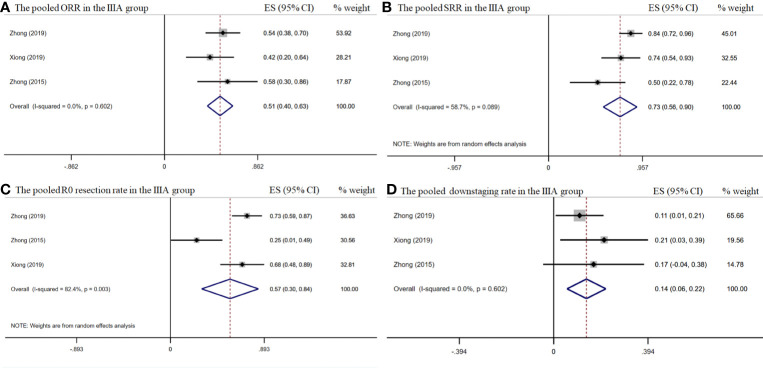
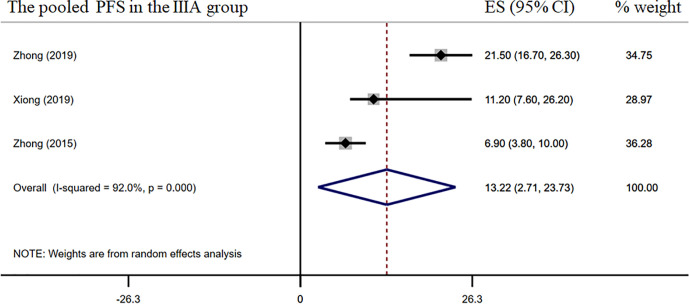
Results: A total of five, phase II, prospective, clinical trials involving 124 patients with resectable or potentially resectable EGFR-mutant NSCLC treated with neoadjuvant erlotinib or gefitinib treatment were included in this pooled analysis. The median neoadjuvant medication time was 42 (range, 21-56) days and the median time of response evaluation was 45 (range, 42-56) days. The pooled ORR was 58.5% [95% confidence interval (CI), 45.5%-71.8%] and the surgical resection and complete resection (R0) rates were 79.9% (95% CI, 65.3%-94.5%) and 64.3% (95% CI, 43.8%-84.8%), respectively. In the stage IIIA subgroup (n = 68), the pooled ORR, SRR, and R0 rate were 51.4%, 72.9%, and 57.0%, respectively, while the downstaging and pCR rates were 14.0% and 0.0%, respectively. The pooled median PFS and overall survival were 13.2 and 41.9 months, respectively. Of the most common grade 3/4 adverse events in the overall group, the incidences of hepatotoxicity and skin rash were 5.3% and 14.7%, respectively. The most commonly reported postoperative complications were lung infection, arrhythmia, and pneumothorax.
Conclusion: Neoadjuvant EGFR-TKI therapy provides a feasible treatment modality for patients with resectable or potentially resectable EGFR-mutant NSCLC, with satisfactory surgical outcomes and low toxicity. Although further phase III clinical trials are needed to confirm these findings, it is necessary to explore the feasibility of a more effective EGFR-TKI combination neoadjuvant therapy given the modest downgrade and pCR rates for EGFR-TKI alone.
Keywords: efficacy; epidermal growth factor receptor-tyrosine kinase inhibitors; neoadjuvant; non-small cell lung cancer; safety.
Copyright © 2021 Sun, Guo, Song, Wang, Zhang, Huang, Zhao, Jing, Han and Ma.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Kwiatkowski DJ, Rusch VW, Chaft JE, Johnson BE, Nicholas A, Wistubaet II, et al. Neoadjuvant atezolizumab in resectable non-small cell lung cancer (NSCLC): Interim analysis and biomarker data from a multicenter study (LCMC3). J Clin Oncol (2019) 37(suppl; abstr 8503):8503-8503. 10.1200/JCO.2019.37.15_suppl.8503 - DOI
-
- Cascone T, William WN, Weissferdt A, Lin HY, Leung CH, Carter BW, et al. Neoadjuvant nivolumab (N) or nivolumab plus ipilimumab (NI) for resectable non-small cell lung cancer (NSCLC): Clinical and correlative results from the NEOSTAR study. J Clin Oncol (2019) 37(suppl; abstr 8504):8504-8504. 10.1200/JCO.2019.37.15_suppl.8504 - DOI
-
- Zhong WZ, Chen KN, Chen C, Gu CD, Wang J, Yang XN, et al. Erlotinib versus gemcitabine plus cisplatin as neoadjuvant treatment of stage IIIA-N2 EGFR-mutant non-small-cell lung cancer (EMERGING-CTONG 1103): A randomized phase II study. J Clin Oncol (2019) 37(25):2235–45. 10.1200/JCO.19.00075 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous