

Modified procedure for prolapse and hemorrhoids: Lower recurrence, higher satisfaction
- PMID: 33511170
- PMCID: PMC7809675
- DOI: 10.12998/wjcc.v9.i1.36
Modified procedure for prolapse and hemorrhoids: Lower recurrence, higher satisfaction
Abstract
Background: Hemorrhoidal prolapse is a common benign disease with a high incidence. The treatment procedure for prolapse and hemorrhoids (PPH) remains an operative method used for internal hemorrhoid prolapse. Although it is related to less pos-operative pain, faster recovery and shorter hospital stays, the postoperative recurrence rate is higher than that of the Milligan-Morgan hemorrhoidectomy (MMH). We have considered that recurrence could be due to shortage of the pulling-up effect. This issue may be overcome by using lower purse-string sutures [modified-PPH (M-PPH)].
Aim: To compare the therapeutic effects and the patients' satisfaction after M-PPH, PPH and MMH.
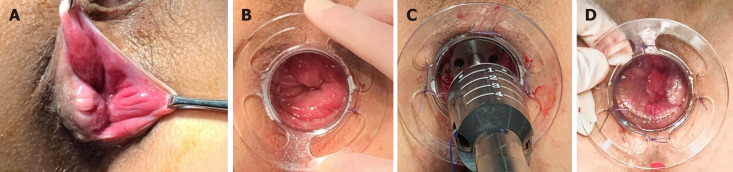
Methods: This retrospective cohort study included 1163 patients (M-PPH, 461; original PPH, 321; MMH, 381) with severe hemorrhoids (stage III/IV) who were admitted to The 2nd Affiliated Hospital and Yuying Children's Hospital of Wenzhou Medical University from 2012 to 2014. Early postoperative complications, efficacy, postoperative anal dysfunction and patient satisfaction were compared among the three groups. Established criteria were used to assess short- and long-term postoperative complications. A visual analog scale was used to evaluate postoperative pain. Follow-up was conducted 5 years postoperatively.
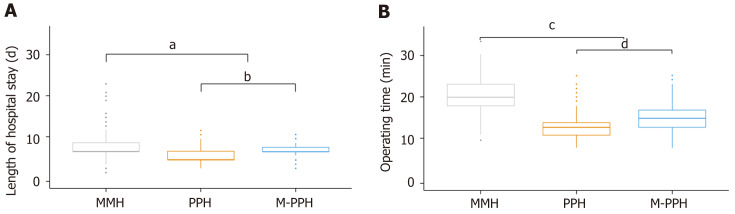
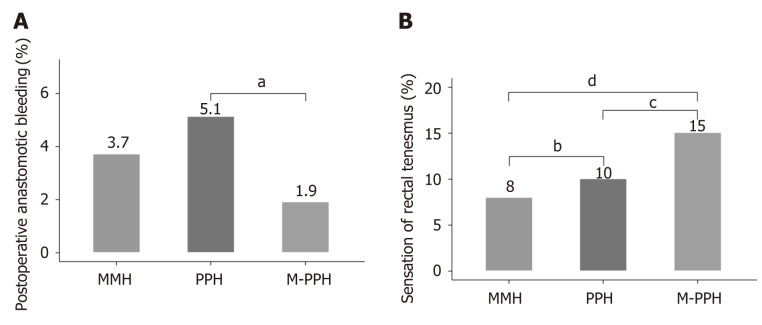
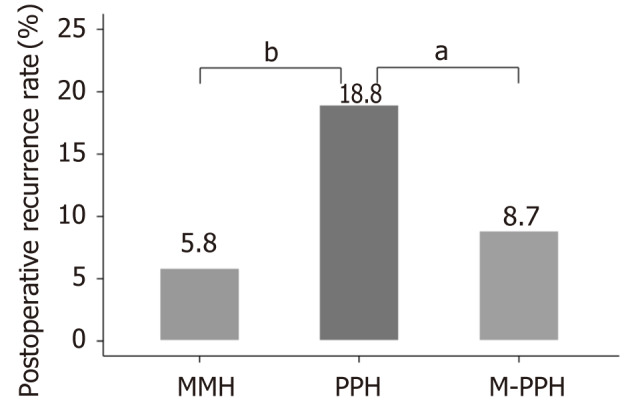
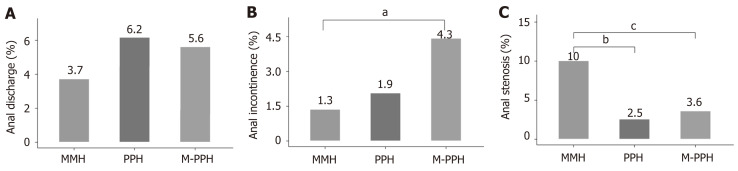
Result: Length of hospital stay and operating time were significantly longer in the MMH group (8.05 ± 2.50 d, 19.98 ± 4.21 min; P < 0.0001) than in other groups. The incidence of postoperative anastomotic bleeding was significantly lower after M-PPH than after PPH or MMH (1.9%, 5.1% and 3.7%; n = 9, 16 and 14; respectively). There was a significantly higher rate of sensation of rectal tenesmus after M-PPH than after MMH or PPH (15%, 8% and 10%; n = 69, 30 and 32; respectively). There was a significantly lower rate of recurrence after M-PPH than after PPH (8.7% and 18.8%, n = 40 and 61; P < 0.0001). The incidence of postoperative anal incontinence differed significantly only between the MMH and M-PPH groups (1.3% and 4.3%, n = 5 and 20; P = 0.04). Patient satisfaction was significantly greater after M-PPH than after other surgeries.
Conclusion: M-PPH has many advantages for severe hemorrhoids (Goligher stage III/IV), with a low rate of anastomotic bleeding and recurrence and a very high rate of patient satisfaction.
Keywords: Hemorrhoids; Milligan-Morgan hemorrhoidectomy; Patient satisfaction; Postoperative complications; Procedure for prolapse and hemorrhoids; Recurrence.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All of the authors have no conflict of interest related to the manuscript.
Figures
References
-
- Haas PA, Haas GP, Schmaltz S, Fox TA Jr. The prevalence of hemorrhoids. Dis Colon Rectum. 1983;26:435–439. - PubMed
-
- Zhang G, Liang R, Wang J, Ke M, Chen Z, Huang J, Shi R. Network meta-analysis of randomized controlled trials comparing the procedure for prolapse and hemorrhoids, Milligan-Morgan hemorrhoidectomy and tissue-selecting therapy stapler in the treatment of grade III and IV internal hemorrhoids(Meta-analysis) Int J Surg. 2020;74:53–60. - PubMed
-
- Anorectal Branch of China Association of Chinese Medicine. The latest results of the national epidemic survey of anorectal diseases have been released. Shijie Zhongxiyi Jiehe Zazhi. 2015;10:1489.
-
- Goligher JC. Surgery of the anus rectum and colon. 4th edition. London: Bailliere, Tindall 1980: 93-149.
-
- Milligan ET, Morgan CN, Jones LE, Officer R. Surgical anatomy of the anal canal and operative treatment of haemorrhoids. Lancet. 1937;2:1119–1124.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
