

Simulating the Fiscal Impact of Anti-Obesity Medications as an Obesity Reduction Strategy
- PMID: 33511897
- PMCID: PMC7970686
- DOI: 10.1177/0046958021990516
Simulating the Fiscal Impact of Anti-Obesity Medications as an Obesity Reduction Strategy
Abstract
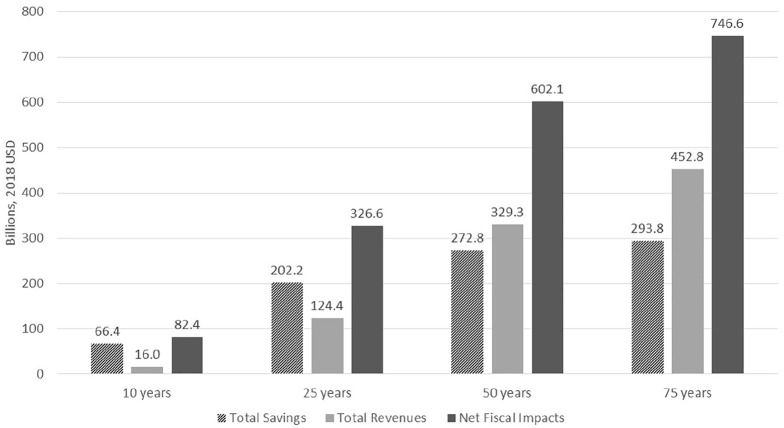
While substantial public health investment in anti-smoking initiatives has had demonstrated benefits on health and fiscal outcomes, similar investment in reducing obesity has not been undertaken, despite the substantial burden obesity places on society. Anti-obesity medications (AOMs) are poorly prescribed despite evidence that weight loss is not sustained using other strategies alone.We used a simulation model to estimate the potential impact of 100% uptake of AOMs on Medicare and Medicaid spending, disability payments, and taxes collected relative to status quo with negligible AOM use. Relative to status quo, AOM use simulation would result in Medicare and Medicaid savings of $231.5 billion and $188.8 billion respectively over 75 years. Government tax revenues would increase by $452.8 billion. Overall, the net benefit would be $746.6 billion. Anti-smoking efforts have had substantial benefits for society. A similar investment in obesity reduction, including broad use of AOMs, should be considered.
Keywords: Medicaid; Medicare; anti-obesity agents; economic modeling; health policy; microsimulation; obesity; public health; weight loss.
Conflict of interest statement
Figures
References
-
- Center for Disease Control and Prevention. Obesity and Overweight. 2016. Accessed November 14, 2019. https://www.cdc.gov/nchs/fastats/obesity-overweight.htm
-
- Wang YC, Pamplin J, Long MW, Ward ZJ, Gortmaker SL, Andreyeva T. Severe obesity in adults cost state medicaid programs nearly $8 billion in 2013. Health Aff (Project Hope). 2015;34(11):1923-1931. - PubMed
-
- Apovian CM. Obesity: definition, comorbidities, causes, and burden. Am J Manag Care. 2016;22(7 Suppl):s176-s185. - PubMed
-
- Allen L, Thorpe K, Joski P. The effect of obesity and chronic conditions on medicare spending, 1987-2011. Pharmacoeconomics. 2015;33(7):691-697. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
