

Simulated Adoption of 2019 Community-Acquired Pneumonia Guidelines Across 114 Veterans Affairs Medical Centers: Estimated Impact on Culturing and Antibiotic Selection in Hospitalized Patients
- PMID: 33512530
- PMCID: PMC12098260
- DOI: 10.1093/cid/ciaa1604
Simulated Adoption of 2019 Community-Acquired Pneumonia Guidelines Across 114 Veterans Affairs Medical Centers: Estimated Impact on Culturing and Antibiotic Selection in Hospitalized Patients
Abstract
Background: The 2019 American Thoracic Society/Infectious Diseases Society of America guidelines for community-acquired pneumonia (CAP) revised recommendations for culturing and empiric broad-spectrum antibiotics. We simulated guideline adoption in Veterans Affairs (VA) inpatients.
Methods: For all VA acute hospitalizations for CAP from 2006-2016 nationwide, we compared observed with guideline-expected proportions of hospitalizations with initial blood and respiratory cultures obtained, empiric antibiotic therapy with activity against methicillin-resistant Staphylococcus aureus (anti-MRSA) or Pseudomonas aeruginosa (antipseudomonal), empiric "overcoverage" (receipt of anti-MRSA/antipseudomonal therapy without eventual detection of MRSA/P. aeruginosa on culture), and empiric "undercoverage" (lack of anti-MRSA/antipseudomonal therapy with eventual detection on culture).
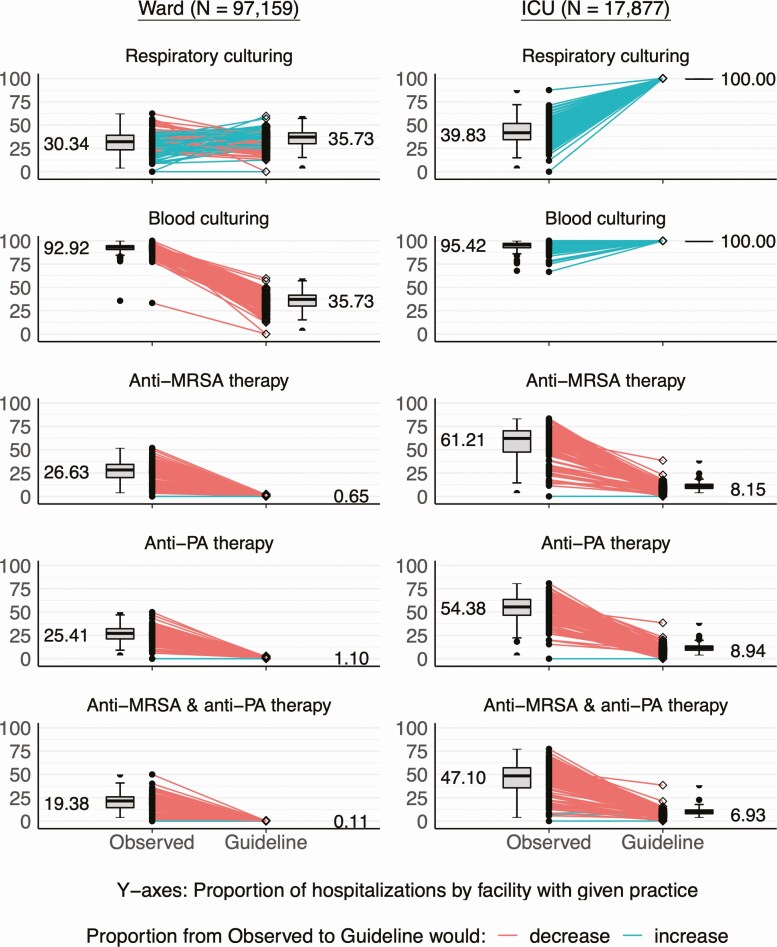
Results: Of 115 036 CAP hospitalizations over 11 years, 17 877 (16%) were admitted to an intensive care unit (ICU). Guideline adoption would slightly increase respiratory culture (30% to 36%) and decrease blood culture proportions (93% to 36%) in hospital wards and increase both respiratory (40% to 100%) and blood (95% to 100%) cultures in ICUs. Adoption would decrease empiric selection of anti-MRSA (ward: 27% to 1%; ICU: 61% to 8%) and antipseudomonal (ward: 25% to 1%; ICU: 54% to 9%) therapies. This would correspond to greatly decreased MRSA overcoverage (ward: 27% to 1%; ICU: 56% to 8%), slightly increased MRSA undercoverage (ward: 0.6% to 1.3%; ICU: 0.5% to 3.3%), with similar findings for P. aeruginosa. For all comparisons, P < .001.
Conclusions: Adoption of the 2019 CAP guidelines in this population would substantially change culturing and empiric antibiotic selection practices, with a decrease in overcoverage and slight increase in undercoverage for MRSA and P. aeruginosa.
Keywords: empiric therapy; guideline; pneumonia.
Published by Oxford University Press for the Infectious Diseases Society of America 2021.
Figures

References
-
- Centers for Disease Control and Prevention. Underlying cause of death 1999–2015 on CDC WONDER online database. Released December, 2016. Available at: http://wonder.cdc.gov/ucd-icd10.html. Accessed 23 October 2017.
-
- Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 2012; 67:71–9. - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med 2010; 38:1045–53. - PubMed
-
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 2005; 171:388–416. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
