

Inverted internal limiting membrane flap technique in eyes with large idiopathic full-thickness macular hole: long-term functional and morphological outcomes
- PMID: 33512612
- PMCID: PMC8277619
- DOI: 10.1007/s00417-021-05082-7
Inverted internal limiting membrane flap technique in eyes with large idiopathic full-thickness macular hole: long-term functional and morphological outcomes
Abstract
Purpose: To investigate morphological and functional outcomes of the inverted internal limiting membrane (I-ILM) flap technique in large (≥ 400 μm) idiopathic full-thickness macular holes (FTMH) over a follow-up period of 12 months.
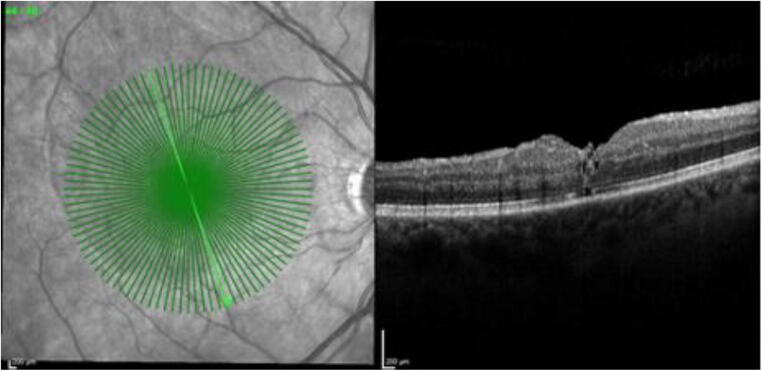
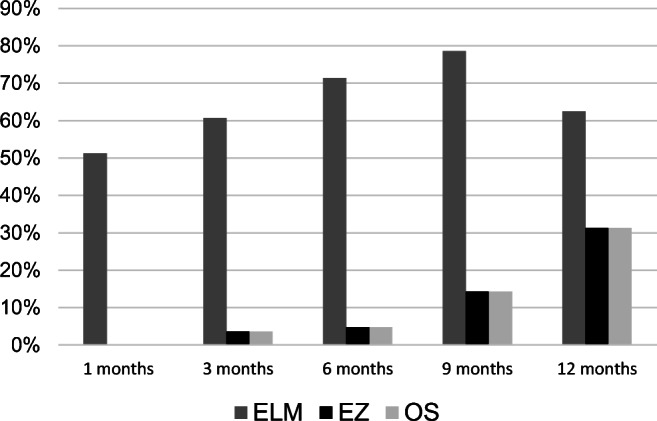
Methods: In this retrospective study, 55 eyes of 54 consecutive patients were enrolled. Best-corrected visual acuity (BCVA) and spectral-domain optical coherence tomography (SD-OCT, Heidelberg, Spectralis) were performed preoperatively as well as 1, 3, 6, 9, and 12 months postoperatively. Special focus was put on the reintegration of outer retinal layers and the different ILM flap appearances.
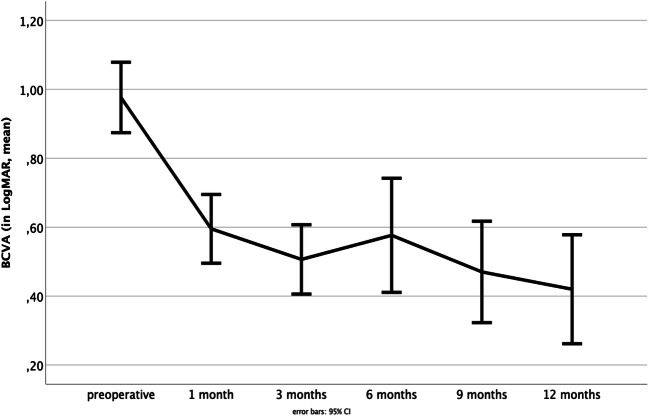
Results: FTMH closure rate was 100% (55/55). BCVA significantly improved over the follow-up period of 12 months from 0.98 ± 0.38 LogMAR preoperatively to 0.42 ± 0.33 LogMAR at 12 months postoperatively (p < 0.001). There was no significant correlation between the three different ILM flap appearances and BCVA. Better preoperative BCVA, complete restoration of the external limiting membrane (ELM), higher macular hole index (MHI), and smaller MH base diameter were associated with higher improvement of BCVA.
Conclusion: Our study highlights the favorable morphological and functional outcomes of the I-ILM flap technique in the short as well as in the long term. While complete ELM restoration revealed to be an important factor for improvement in BCVA, the different postoperative ILM flap appearances seem not to be related to BCVA.
Keywords: External limiting membrane; Flap appearance; Inverted internal limiting membrane flap technique; Large macular hole; Macular hole index; Spectral-domain optical coherence tomography.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




Similar articles
-
Inverted internal limiting membrane flap technique versus complete internal limiting membrane peeling in large macular hole surgery: a comparative study.BMC Ophthalmol. 2020 Jan 6;20(1):11. doi: 10.1186/s12886-019-1294-8. BMC Ophthalmol. 2020. PMID: 31907015 Free PMC article.
-
[Vitrectomy and iOCT-assisted inverted ILM flap technique in patients with full thickness macular holes].Ophthalmologe. 2019 Jul;116(7):617-624. doi: 10.1007/s00347-018-0769-y. Ophthalmologe. 2019. PMID: 30105564 German.
-
Visual improvement and regeneration of retinal layers in eyes with small, medium, and large idiopathic full-thickness macular holes treated with the inverted internal limiting membrane flap technique over a period of 12 months.Graefes Arch Clin Exp Ophthalmol. 2022 Oct;260(10):3161-3171. doi: 10.1007/s00417-022-05676-9. Epub 2022 Apr 27. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 35475915 Free PMC article.
-
Comparative efficacy evaluation of inverted internal limiting membrane flap technique and internal limiting membrane peeling in large macular holes: a systematic review and meta-analysis.BMC Ophthalmol. 2020 Jan 8;20(1):14. doi: 10.1186/s12886-019-1271-2. BMC Ophthalmol. 2020. PMID: 31914954 Free PMC article.
-
Flap technique-assisted surgeries for advanced retinitis pigmentosa complicated with macular hole: a case report and literature review.BMC Ophthalmol. 2021 Sep 6;21(1):322. doi: 10.1186/s12886-021-02082-3. BMC Ophthalmol. 2021. PMID: 34488687 Free PMC article. Review.
Cited by
-
Microperimetric evaluation and predictive factors of visual recovery after successful inverted internal limiting membrane-flap technique for macular hole in high myopic eyes.Front Med (Lausanne). 2023 Nov 23;10:1276502. doi: 10.3389/fmed.2023.1276502. eCollection 2023. Front Med (Lausanne). 2023. PMID: 38076261 Free PMC article.
-
[iOCT in clinical use : Correlation of intraoperative morphology and postoperative visual outcome in patients with full thickness macular hole].Ophthalmologe. 2022 May;119(5):491-496. doi: 10.1007/s00347-021-01527-w. Epub 2021 Nov 4. Ophthalmologe. 2022. PMID: 34735612 Free PMC article. German.
-
360° inverted internal limiting membrane flap technique for idiopathic macular holes ≤ 250 µm, > 250 and ≤ 400 µm, and > 400 µm.Graefes Arch Clin Exp Ophthalmol. 2022 Jul;260(7):2183-2190. doi: 10.1007/s00417-022-05587-9. Epub 2022 Feb 19. Graefes Arch Clin Exp Ophthalmol. 2022. PMID: 35182187 Clinical Trial.
-
Yin-Yang Staining Technique to Create a Nonstained Internal Limiting Membrane Flap to Cover Large Idiopathic Macular Holes.J Vitreoretin Dis. 2024 Dec 21:24741264241308486. doi: 10.1177/24741264241308486. Online ahead of print. J Vitreoretin Dis. 2024. PMID: 39711690 Free PMC article.
-
Changes in vascular density in the macula after pars plana vitrectomy for idiopathic macular hole with macular peeling and one type of flap.Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2024 Sep;168(3):248-255. doi: 10.5507/bp.2023.017. Epub 2023 Apr 28. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2024. PMID: 37114702
References
-
- Duker J, Kaiser P, Binder S, de Smet M, Gaudric A, Reichel E, Sadda S, Sebag J, Spaide R, Stalmans P. The international vitreomacular traction study group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120:2611–2619. doi: 10.1016/j.ophtha.2013.07.042. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
