

Randomized, Placebo Controlled Trial of Experimental Hookworm Infection for Improving Gluten Tolerance in Celiac Disease
- PMID: 33512796
- PMCID: PMC7678792
- DOI: 10.14309/ctg.0000000000000274
Randomized, Placebo Controlled Trial of Experimental Hookworm Infection for Improving Gluten Tolerance in Celiac Disease
Abstract
Introduction: Celiac disease is an autoimmune disorder where intestinal immunopathology arises after gluten consumption. Previous studies suggested that hookworm infection restores gluten tolerance; however, these studies were small (n = 12) and not placebo controlled.
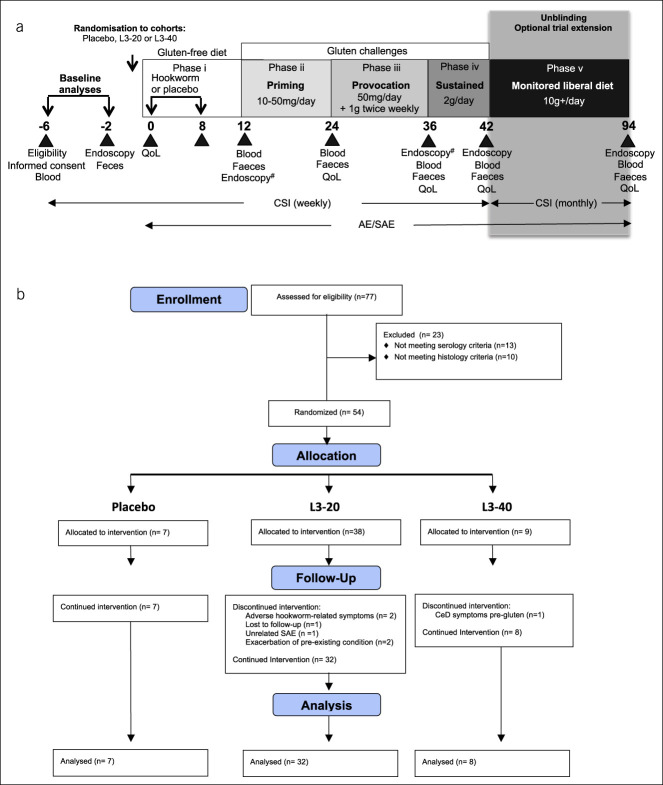
Methods: We undertook a randomized, placebo-controlled trial of hookworm infection in 54 people with celiac disease. The 94-week study involved treatment with either 20 or 40 Necator americanus third-stage larvae (L3-20 or L3-40) or placebo, followed by escalating gluten consumption (50 mg/d for 12 weeks, 1 g intermittent twice weekly for 12 weeks, 2 g/d sustained for 6 weeks, liberal diet for 1 year).
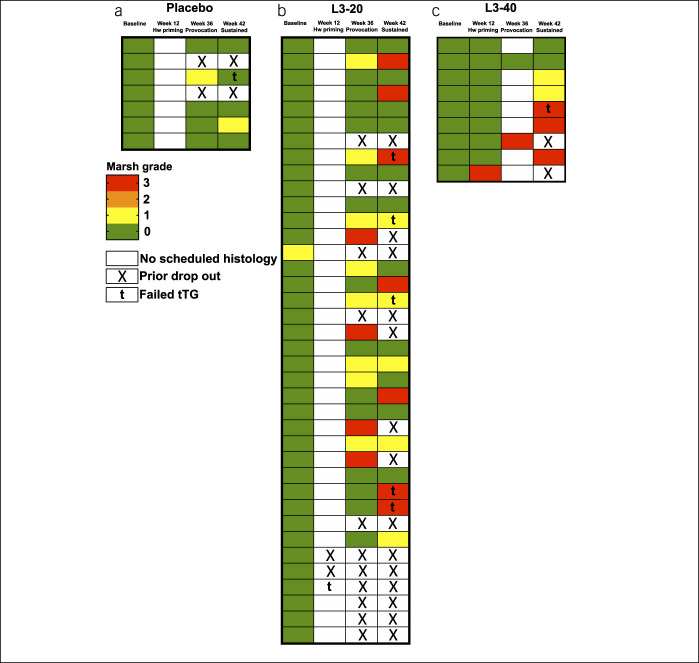
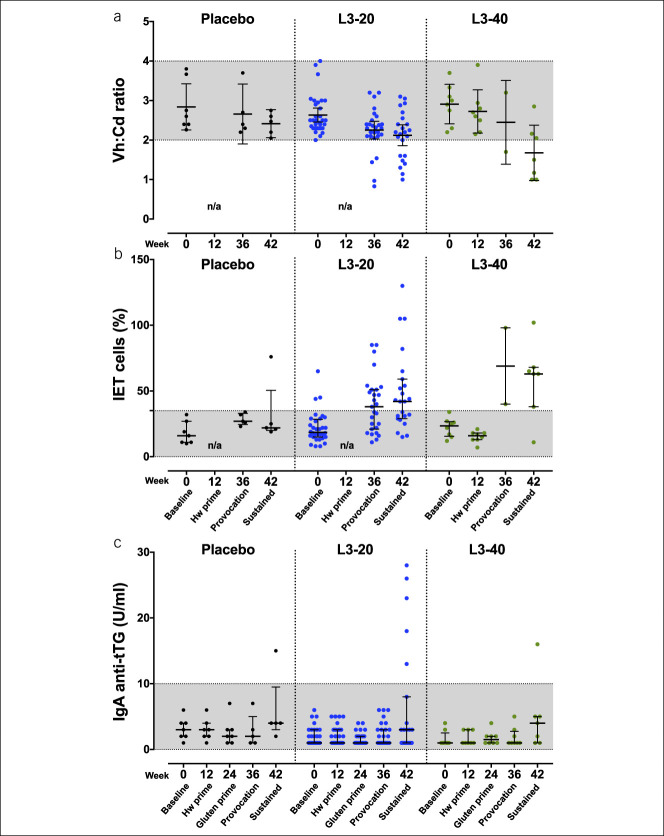
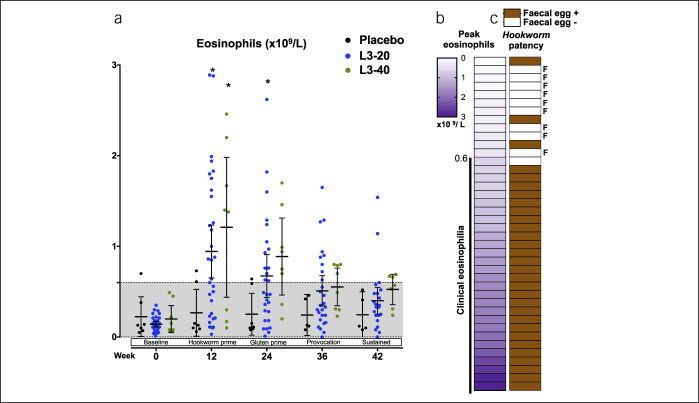
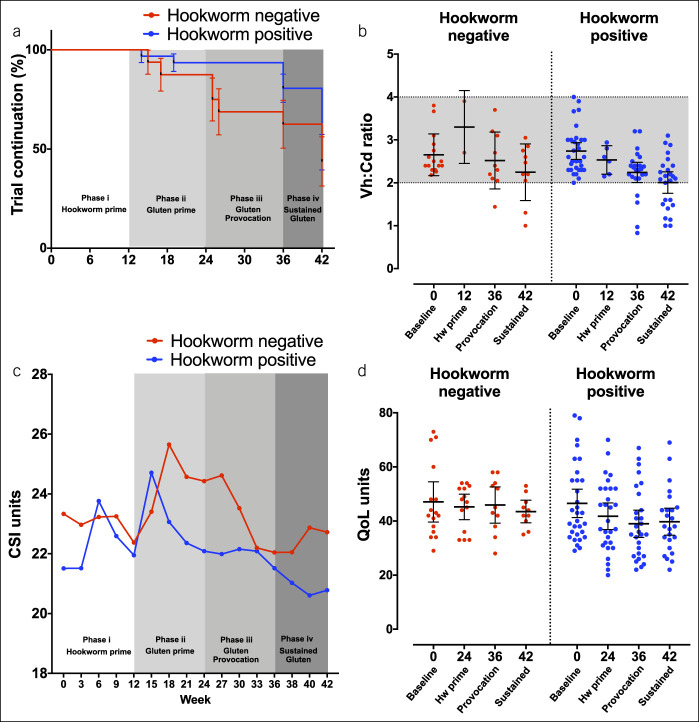
Results: Successful study completion rates at week 42 (primary outcome) were similar in each group (placebo: 57%, L3-20: 37%, and L3-40: 44%; P = 0.61), however gluten-related adverse events were significantly reduced in hookworm-treated participants: Median (range) adverse events/participant were as follows: placebo, 4 (1-9); L3-20, 1 (0-9); and L3-40, 0 (0-3) (P = 0.019). Duodenal villous height:crypt depth deteriorated similarly compared with their enrolment values in each group (mean change [95% confidence interval]: placebo, -0.6 [-1.3 to 0.2]; L3-20, -0.5 [-0.8 to 0.2]; and L3-40, -1.1 [-1.8 to 0.4]; P = 0.12). A retrospective analysis revealed that 9 of the 40 L3-treated participants failed to establish hookworm infections. Although week 42 completion rates were similar in hookworm-positive vs hookworm-negative participants (48% vs 44%, P = 0.43), quality of life symptom scores were lower in hookworm-positive participants after intermittent gluten challenge (mean [95% confidence interval]: 38.9 [33.9-44] vs 45.9 [39.2-52.6]).
Discussion: Hookworm infection does not restore tolerance to sustained moderate consumption of gluten (2 g/d) but was associated with improved symptom scores after intermittent consumption of lower, intermittent gluten doses.
Conflict of interest statement
Figures
References
-
- Qiao SW, Iversen R, Raki M, et al. The adaptive immune response in celiac disease. Semin Immunopathol 2012;34:523–40. - PubMed
-
- Abadie V, Discepolo V, Jabri B. Intraepithelial lymphocytes in celiac disease immunopathology. Semin Immunopathol 2012;34:551–66. - PubMed
-
- Di Sabatino A, Vanoli A, Giuffrida P, et al. The function of tissue transglutaminase in celiac disease. Autoimmun Rev 2012;11:746–53. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
