A multicentered study on efficiency of noninvasive ventilation procedures (SAFE-NIV)
- PMID: 33512813
- PMCID: PMC8283467
- DOI: 10.3906/sag-2004-35
A multicentered study on efficiency of noninvasive ventilation procedures (SAFE-NIV)
Abstract
Background/aim: To characterize the clinical course of noninvasive positive pressure ventilation (NIPPV) and high flow humidified nasal cannula ventilation (HFNC) procedures; perform risk analysis for ventilation failure.
Material and methods: This prospective, multi-centered, observational study was conducted in 352 PICU admissions (1 month-18 years) between 2016 and 2017. SPSS-22 was used to assess clinical data, define thresholds for ventilation parameters and perform risk analysis.
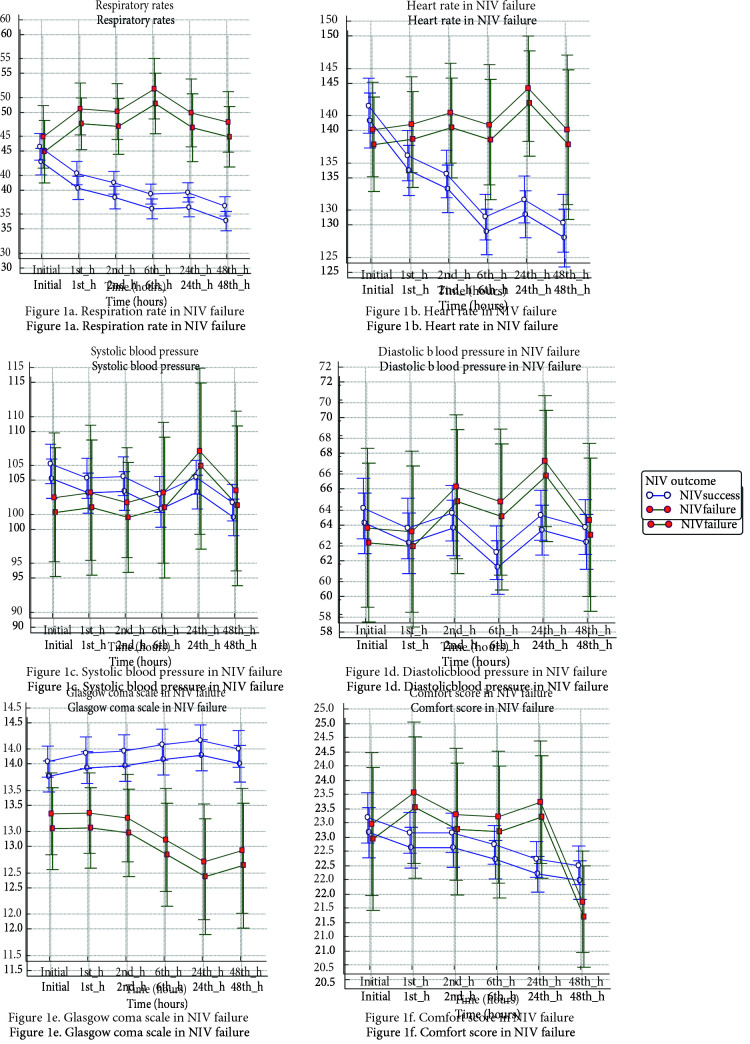
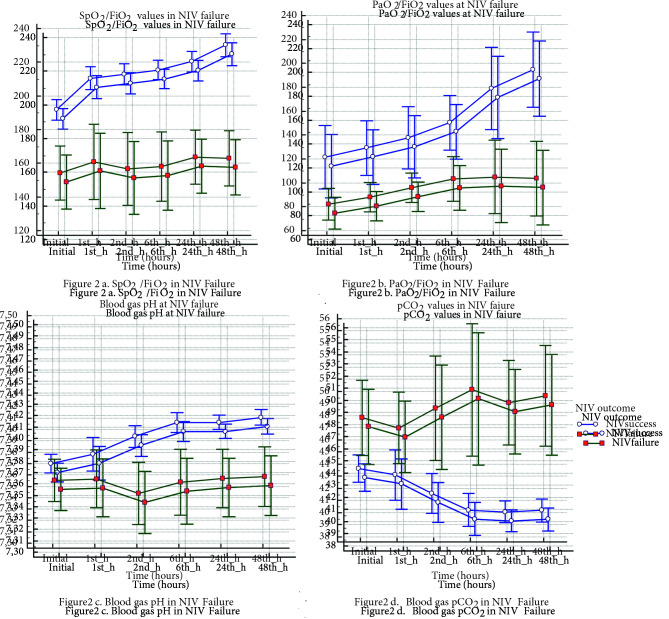
Results: Patient age, onset of disease, previous intubation and hypoxia influenced the choice of therapy mode: NIPPV was preferred in older children (p = 0.002) with longer intubation (p < 0.001), ARDS (p = 0.001), lower respiratory tract infections (p < 0.001), chronic respiratory disease, (p = 0.005), malignancy (p = 0.048) and immune deficiency (p = 0.026). The failure rate was 13.4%. sepsis, ARDS, prolonged intubation, and use of nasal masks were associated with NIV failure (p = 0.001, p < 0.001, p < 0.001, p = 0.025). The call of intubation or re-intubation was given due to respiratory failure in twenty-seven (57.5%), hemodynamic instability in eight (17%), bulbar dysfunction or aspiration in 5 (10.6%), neurological deterioration in 4 (8.5%) and developing ARDS in 3 (6.4%) children. A reduction of less than 10% in the respiration within an hour increased the odds of failure by 9.841 times (OR: 9.841, 95% CI: 2.0021–48.3742). FiO2 > 55% at 6th hours and PRISM-3 >8 were other failure predictors. Of the 9.9% complication rate, the most common complication was pressure ulcerations (4.8%) and mainly observed when using full-face masks (p = 0.047). Fifteen (4.3%) patients died of miscellaneous causes. Tracheostomy cannulation was performed on 16 children due to prolonged mechanical ventilation (8% in NIPPV, 2.6% in HFNC)
Conclusion: Absence of reduction in the respiration rate within an hour, FiO2 requirement >55% at 6th hours and PRISM-3 score >8 predict NIV failure.
Keywords: HFNC; children; respiratory failure; noninvasive positive pressure ventilation.
This work is licensed under a Creative Commons Attribution 4.0 International License.
Conflict of interest statement
none declared
Figures
References
-
- Determination of the effects of the canola oil on the performance and emission characteristics of the diesel engine. Master Thesis . 2006.
-
- Wing R Armsby CC Non-invasive ventilation in pediatric acute respiratory illness. Clinical Pediatric Emergency Medicine . 2015;16:154–161.
-
- Fioretto JR Ribeiro CF Carpi MF Bonatto RC Comparison between noninvasive mechanical ventilation and standard oxygen therapy in children up to 3 years old with respiratory failure after extubation: a pilot prospective randomized clinical study. Pediatric Critical Care Medicine . 2015;16:124–130. - PubMed
-
- Fedor KL Noninvasive respiratory support in infants and children. Respiratory Care . 2017;62:699–717. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous