

The feasibility and reliability of actigraphy to monitor sleep in intensive care patients: an observational study
- PMID: 33514414
- PMCID: PMC7844945
- DOI: 10.1186/s13054-020-03447-8
The feasibility and reliability of actigraphy to monitor sleep in intensive care patients: an observational study
Abstract
Background: Sleep amongst intensive care patients is reduced and highly fragmented which may adversely impact on recovery. The current challenge for Intensive Care clinicians is identifying feasible and accurate assessments of sleep that can be widely implemented. The objective of this study was to investigate the feasibility and reliability of a minimally invasive sleep monitoring technique compared to the gold standard, polysomnography, for sleep monitoring.
Methods: Prospective observational study employing a within subject design in adult patients admitted to an Intensive Care Unit. Sleep monitoring was undertaken amongst minimally sedated patients via concurrent polysomnography and actigraphy monitoring over a 24-h duration to assess agreement between the two methods; total sleep time and wake time.
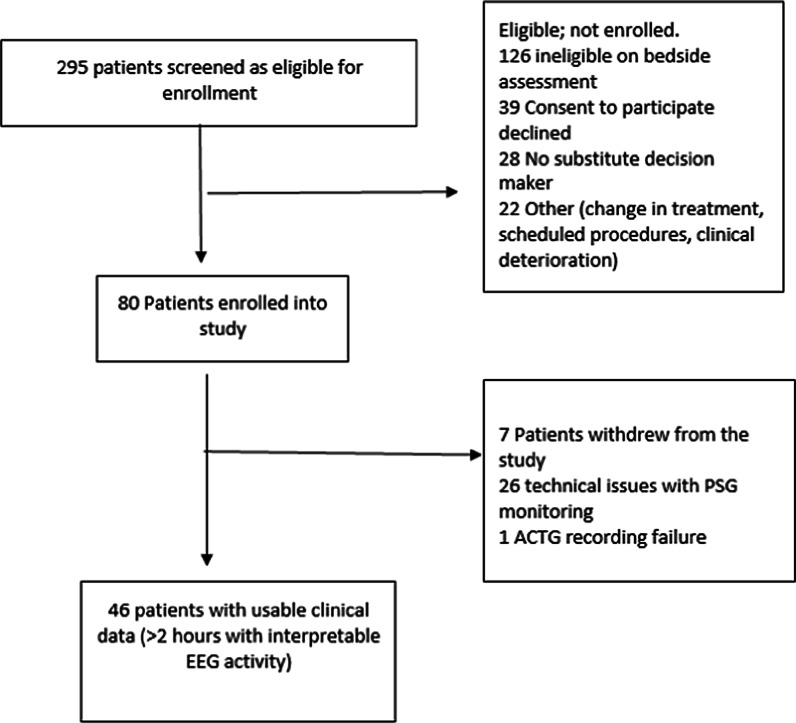
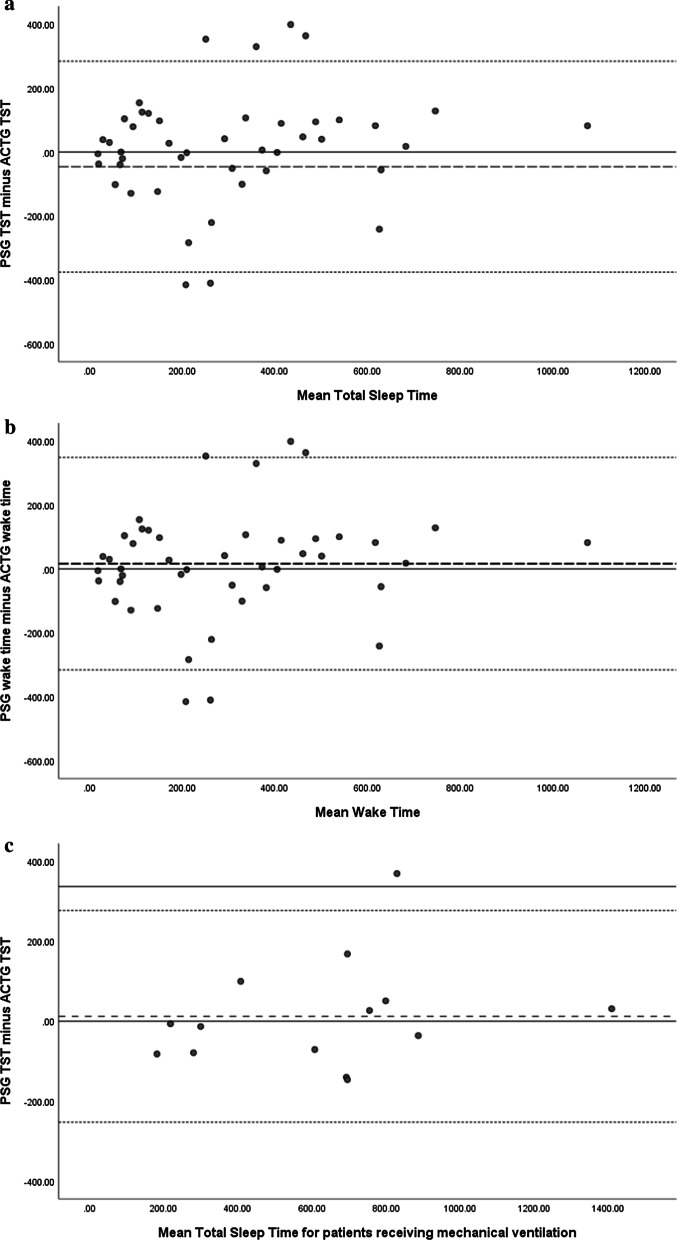
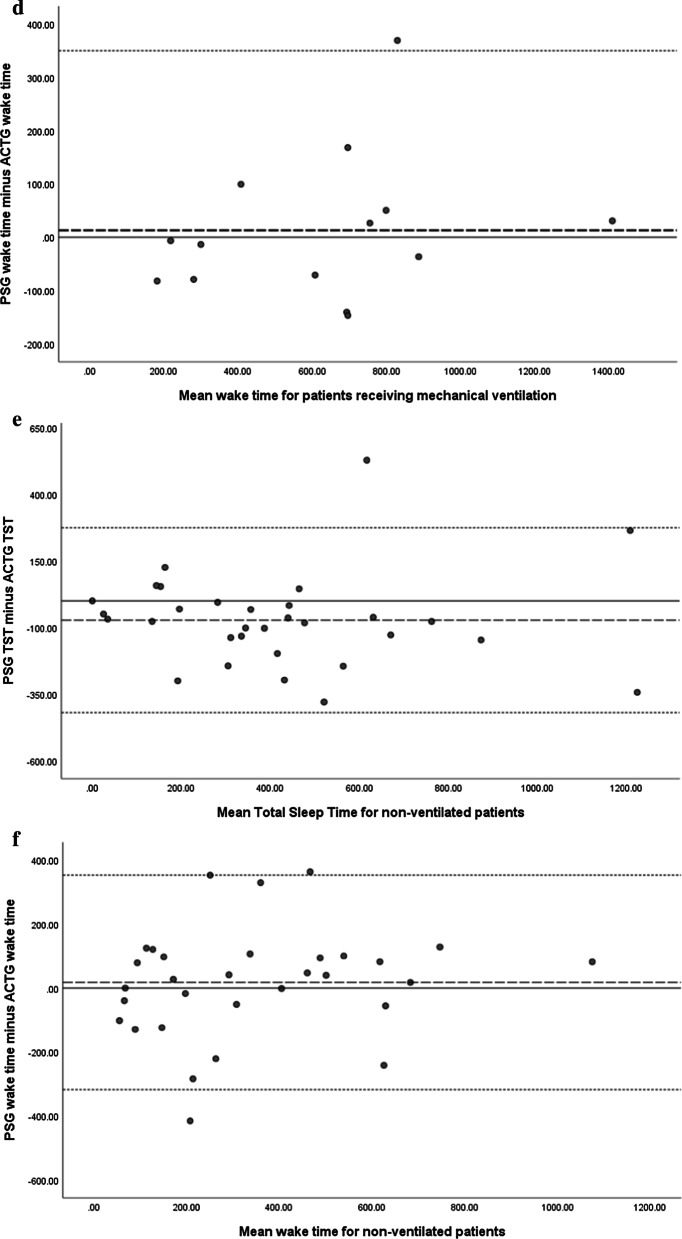
Results: We recruited 80 patients who were mechanically ventilated (24%) and non-ventilated (76%) within the intensive care unit. Sleep was found to be highly fragmented, composed of numerous sleep bouts and characterized by abnormal sleep architecture. Actigraphy was found to have a moderate level of overall agreement in identifying sleep and wake states with polysomnography (69.4%; K = 0.386, p < 0.05) in an epoch by epoch analysis, with a moderate level of sensitivity (65.5%) and specificity (76.1%). Monitoring accuracy via actigraphy was improved amongst non-ventilated patients (specificity 83.7%; sensitivity 56.7%). Actigraphy was found to have a moderate correlation with polysomnography reported total sleep time (r = 0.359, p < 0.05) and wakefulness (r = 0.371, p < 0.05). Bland-Altman plots indicated that sleep was underestimated by actigraphy, with wakeful states overestimated.
Conclusions: Actigraphy was easy and safe to use, provided moderate level of agreement with polysomnography in distinguishing between sleep and wakeful states, and may be a reasonable alternative to measure sleep in intensive care patients. Clinical Trial Registration number ACTRN12615000945527 (Registered 9/9/2015).
Keywords: Actigraphy; Intensive care; Polysomnography; Sleep; Sleep disturbance; Sleep quality.
Conflict of interest statement
Nil competing interests to declare.
Figures
Similar articles
-
Investigating the application of motion accelerometers as a sleep monitoring technique and the clinical burden of the intensive care environment on sleep quality: study protocol for a prospective observational study in Australia.BMJ Open. 2018 Jan 21;8(1):e019704. doi: 10.1136/bmjopen-2017-019704. BMJ Open. 2018. PMID: 29358448 Free PMC article.
-
Actigraphy versus Polysomnography to Measure Sleep in Youth Treated for Craniopharyngioma.Behav Sleep Med. 2020 Sep-Oct;18(5):589-597. doi: 10.1080/15402002.2019.1635133. Epub 2019 Jul 14. Behav Sleep Med. 2020. PMID: 31303059
-
The accuracy of simple, feasible alternatives to polysomnography for assessing sleep in intensive care: An observational study.Aust Crit Care. 2023 May;36(3):361-369. doi: 10.1016/j.aucc.2022.02.004. Epub 2022 Mar 28. Aust Crit Care. 2023. PMID: 35361553
-
Actigraphy to Evaluate Sleep in the Intensive Care Unit. A Systematic Review.Ann Am Thorac Soc. 2018 Sep;15(9):1075-1082. doi: 10.1513/AnnalsATS.201801-004OC. Ann Am Thorac Soc. 2018. PMID: 29944386 Free PMC article.
-
Assessment and Monitoring of Sleep in the Intensive Care Unit.Crit Care Nurs Clin North Am. 2021 Jun;33(2):109-119. doi: 10.1016/j.cnc.2021.01.008. Epub 2021 Apr 24. Crit Care Nurs Clin North Am. 2021. PMID: 34023079 Free PMC article. Review.
Cited by
-
Reduction of the Cycle Time in the Biopsies Diagnosis Through a Simulation Based on the Box Müller Algorithm.Front Public Health. 2022 Apr 4;10:809534. doi: 10.3389/fpubh.2022.809534. eCollection 2022. Front Public Health. 2022. PMID: 35444982 Free PMC article.
-
Translation and Validation of the Richards-Campbell Sleep Questionnaire for Intensive Care Unit Patients in Morocco: Reliability and Validity Assessment.Clocks Sleep. 2025 Jun 23;7(3):31. doi: 10.3390/clockssleep7030031. Clocks Sleep. 2025. PMID: 40700253 Free PMC article.
-
Sleep and mental health in recruit paramedics: a 6-month longitudinal study.Sleep. 2023 Aug 14;46(8):zsad050. doi: 10.1093/sleep/zsad050. Sleep. 2023. PMID: 36861384 Free PMC article.
-
Feasibility and Acceptability of Using Wireless Limited Polysomnography to Capture Sleep Before, During, and After Hospitalization for Patients With Planned Cardiothoracic Surgery.J Cardiovasc Nurs. 2025 May-Jun 01;40(3):E110-E116. doi: 10.1097/JCN.0000000000001092. Epub 2024 Mar 21. J Cardiovasc Nurs. 2025. PMID: 38509035
-
Depressive symptom screening in elderly by passive sensing data of smartphones or smartwatches: A systematic review.PLoS One. 2024 Jun 27;19(6):e0304845. doi: 10.1371/journal.pone.0304845. eCollection 2024. PLoS One. 2024. PMID: 38935797 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
