

Safety and efficacy of intra-arterial fibrinolytics as adjunct to mechanical thrombectomy: a systematic review and meta-analysis of observational data
- PMID: 33514609
- PMCID: PMC8606438
- DOI: 10.1136/neurintsurg-2020-016680
Safety and efficacy of intra-arterial fibrinolytics as adjunct to mechanical thrombectomy: a systematic review and meta-analysis of observational data
Abstract
Background: Achieving the best possible reperfusion is a key determinant of clinical outcome after mechanical thrombectomy (MT). However, data on the safety and efficacy of intra-arterial (IA) fibrinolytics as an adjunct to MT with the intention to improve reperfusion are sparse.
Methods: We performed a PROSPERO-registered (CRD42020149124) systematic review and meta-analysis accessing MEDLINE, PubMed, and Embase from January 1, 2000 to January 1, 2020. A random-effect estimate (Mantel-Haenszel) was computed and summary OR with 95% CI were used as a measure of added IA fibrinolytics versus control on the risk of symptomatic intracranial hemorrhage (sICH) and secondary endpoints (modified Rankin Scale ≤2, mortality at 90 days).
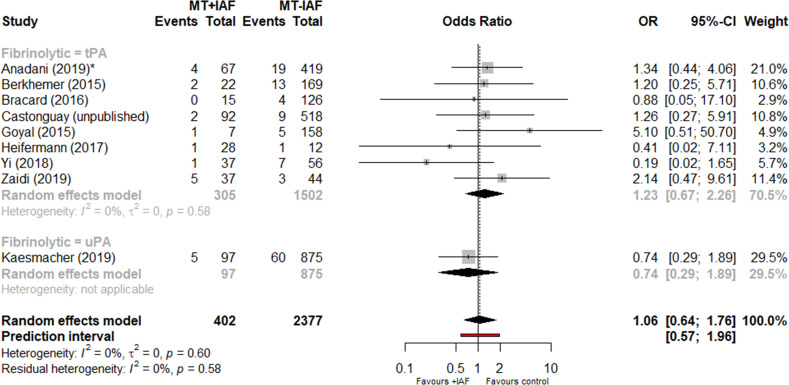
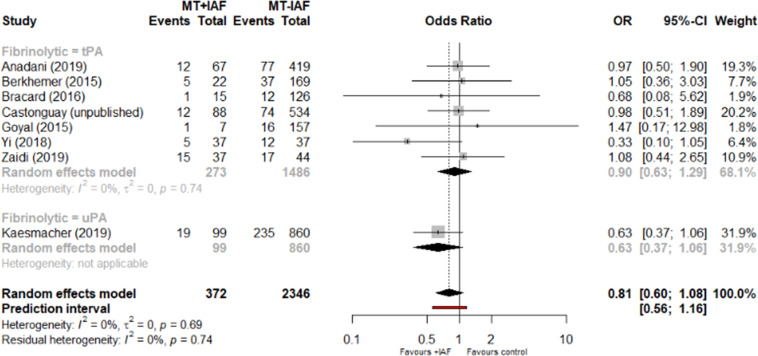
Results: The search identified six observational cohort studies and three observational datasets of MT randomized-controlled trial data reporting on IA fibrinolytics with MT as compared with MT alone, including 2797 patients (405 with additional IA fibrinolytics (100 urokinase (uPA), 305 tissue plasminogen activator (tPA)) and 2392 patients without IA fibrinolytics). Of 405 MT patients treated with additional IA fibrinolytics, 209 (51.6%) received prior intravenous tPA. We did not observe an increased risk of sICH after administration of IA fibrinolytics as adjunct to MT (OR 1.06, 95% CI 0.64 to 1.76), nor excess mortality (0.81, 95% CI 0.60 to 1.08). Although the mode of reporting was heterogeneous, some studies observed improved reperfusion after IA fibrinolytics.
Conclusion: The quality of evidence regarding peri-interventional administration of IA fibrinolytics in MT is low and limited to observational data. In highly selected patients, no increase in sICH was observed, but there is large uncertainty.
Keywords: stroke; thrombectomy; thrombolysis.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Related: UF and JG are global PIs for the SWIFT DIRECT study (Solitaire With the Intention for Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke) supported by Medtronic. Unrelated: JG is a global PI of STAR (Solitaire FR Thrombectomy for Acute Revascularisation Observational study), Clinical Event Committee member of the PROMISE study (European Registry on the ACE Reperfusion Catheters and the Penumbra System in the Treatment of Acute Ischemic Stroke; Penumbra), Consultancy, and receives Swiss National Science Foundation (SNSF) grants for MRI in stroke. UF receives research grants from SNSF and serves as a consultant for Medtronic and Stryker. MA received speaker honoraria from Bayer, Boehringer Ingelheim, and Covidien; advisory board honoraria from Amgen Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Pfizer, Covidien, Daichy Sankyo and Nestlé Health Science; research grant provided by the Swiss Heart Foundation. JK reports grants from SAMW / Bangerter Foundation, the Swiss Stroke Society and non-financial support from Stryker and Pfizer outside the submitted work. DWJD reports funding from the Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, and unrestricted grants from AngioCare BV, Covidien/EV3®, MEDAC Gmbh/LAMEPRO, Penumbra Inc., Top Medical/Concentric, Stryker, Stryker European Operations BV, Medtronic, Thrombolytic Science, LLC and Cerenovus for research, all paid to institution. MG reports licensing agreement for systems of acute stroke diagnosis for GE Healthcare and Consultancy for Medtronic, Stryker, MicroVention and Mentice as well as unrestricted research grant by Stryker for the UNMASK-EVT study. MDH has a patent Systems and Methods for Assisting in Decision-Making and Triaging for Acute Stroke Patients pending to US patent office number 62/086077 and owns stock in Calgary Scientific, Inc—a company that focuses on medical imaging software.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous